Abstract
Keywords: Additive manufacturing; occlusal device; 3D printed resin; print orientation; digital dentistry
Dentistry is undergoing a pronounced digital transformation, with traditional workflows progressively supplanted by advanced three-dimensional technologies, notably additive manufacturing (AM; commonly referred to as 3D printing). AM employs computer-aided design (CAD) data, along with a range of material systems, to fabricate patient-specific devices by successive layer-wise deposition, in contrast to subtractive techniques that produce objects by removing material from prefabricated blocks [1]. Both additive and subtractive manufacturing processes are governed by international standards (ISO), which prescribe criteria for reproducibility, safety, dimensional accuracy and overall quality assurance in dental production [2]. The adoption of 3D printing has expanded markedly across oral and maxillofacial surgery, prosthodontics, and orthodontics, where its capacity for precise, customized fabrication offers clinical and workflow advantages [1,2].
Among orthodontic and restorative adjuncts, occlusal devices (OC) are widely used and have broad interdisciplinary applications, including the treatment of temporomandibular disorders (TMD), support during orthodontic therapy, and prevention of parafunctional damage. Their therapeutic efficacy derives from the redistribution of occlusal forces, the reduction of masticatory muscle hyperactivity and the mitigation of the deleterious sequelae of bruxism and TMD [3]. Conventional subtractive manufacturing (SM), principally milling, requires the fabrication of each device individually, a process that is comparatively time-consuming and generates substantial material waste [3]. By contrast, AM permits the concurrent production of multiple devices in a single build volume, necessitating the post-processing removal of support structures; the principle is used to develop various methods, especially the stereolithography (SLA) is one of the predominant AM modalities employed for device fabrication due to its resolution and material properties [4,5]. The SLA technology uses a laser beam to activate photo-initiators sequentially, resulting in local polymerisation of the directly exposed area. Since the object is manufactured layer by layer, it is anisotropic, meaning that its orientation relative to the printer’s platform during fabrication affects its properties [6]. Research indicates that the orientation of 3D-printed OCs relative to the printer’s build plate can significantly affect various factors. These include printing time, the need for support structures, the volume of material used, and the final product attributes, such as OC fit, surface roughness, wear, and mechanical properties [3,7–9]. Additionally, previous studies reported clinical observations that printing orientation is a determinant of the internal fit of 3D-printed occlusal devices by SLA [8,10,11].
This in vivo study investigates the accuracy of SLA-printed occlusal devices fabricated at 0° and 45° orientations, addressing a gap in research despite known effects of printing orientation, technology, and printer on device accuracy. The primary null hypothesis is that printing orientation does not affect the accuracy of SLA-printed occlusal devices in patients with TMD. The study also compares surface roughness, fit accuracy, wear, and therapeutic effects of 3D-printed vs. traditionally manufactured occlusal devices. The secondary null hypothesis is that 3D-printed occlusal devices are not inferior to traditional devices in therapeutic effects, clinical performance (surface roughness, wear, antagonist tooth abrasion, device fit).
Conducted at the Department of Prosthodontics, Istanbul University, from January to June 2024 (ethical batch number TDK 2024/35910; ClinicalTrials.gov identifier: NCT05955222), this study involved 40 participants who met the following criteria: presence of maxillofacial pain, limited functional movements, a diagnosis of DC/TMD, absence of missing teeth or prostheses, and an age range of 18 to 60 years. A sample size calculation, employing an alpha of 0.05 and a power of 0.95, determined that 10 participants per group were necessary to detect a one-standard-deviation difference in the primary endpoint. Functional assessment involved the clinical examination component of the Turkish DC/TMD form, a validated diagnostic tool (International DC/TMD-Based Research Consortium) [12]. Subjective pain was assessed using a visual analog scale (VAS).
Type IV die-stone gypsum casts (Kulzer GmbH) were created from condensation silicone impressions (Speedex Putty and Light Body; Coltène). Participants were randomly assigned to four groups: conventionally fabricated PMMA occlusal devices (CPMMA), CAD/CAM milled PMMA (MPMMA), 3D-printed at 0 degrees (3D 0°), and 3D-printed at 45 degrees (3D 45°). Group randomization was conducted based on the days of the week. Patients who were examined on Monday were assigned to the PMMA group, those examined on Tuesday were assigned to the MPMMA group, patients examined on Wednesday were assigned to the 3D 0° group, and those examined on Thursday were assigned to the 3D 45° group (workflow detailed in Figure 1). Gypsum casts were digitally scanned (Dental Wings; Dental Wings Inc.) and saved as STL files. Exocad’s Bite Occlusal Module was used to virtually design flat occlusal surface OCs, which then underwent dynamic occlusion adjustment in a virtual articulator. Roland DWX-52D machine was used for the milling group (Roland DGA Corp). Occlusal devices for the conventional group were produced from PMMA-based thermoformable disks [13]. Chairside occlusal adjustments were made with autopolymerizing acrylic resin (Integra acrylic; United Group Dental).
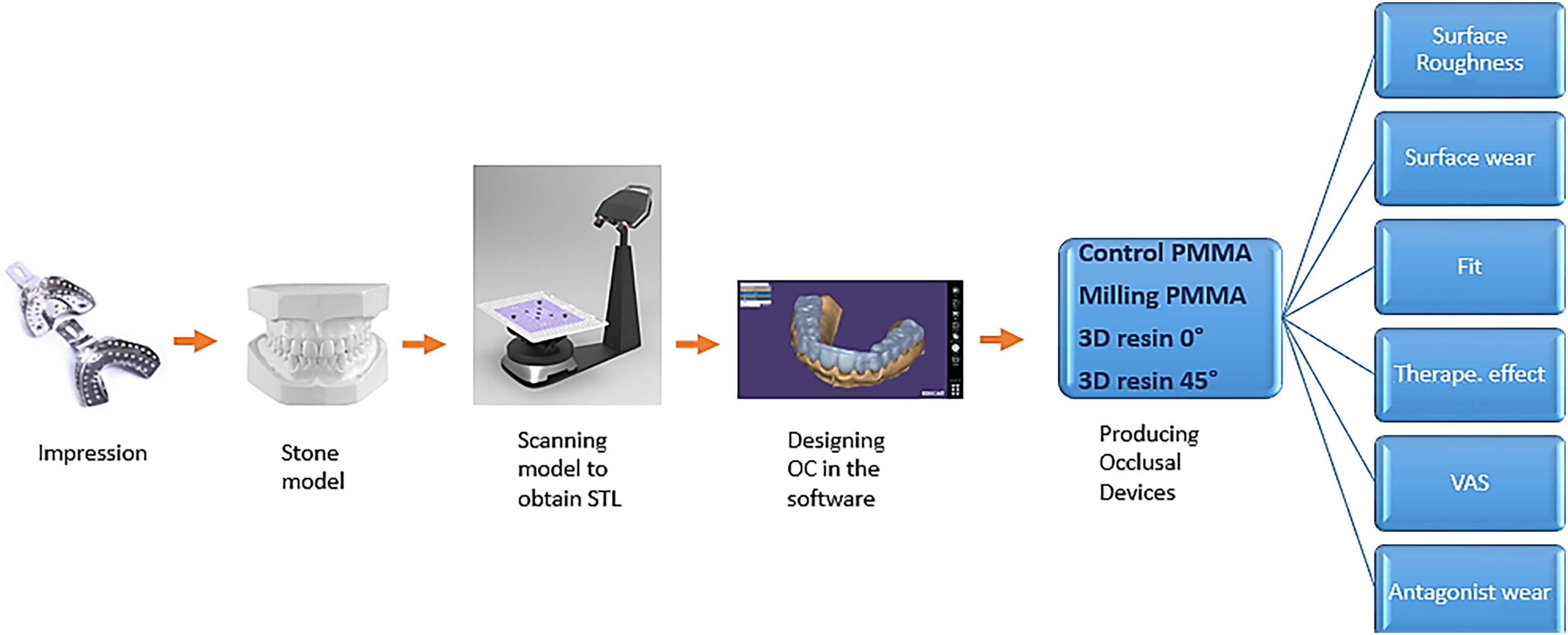
Figure 1. Workflow of the study groups
3D-printed OCs were additively manufactured with components oriented at 0° or 45° (Figure 2), using a 100 μm layer thickness as per manufacturer’s recommendations. Ten OCs per group were printed using Dental LT resin (Formlabs, Sommerville, MA, USA) in a Form 2 printer (Formlabs, MA, USA). Following printing and illumination, OCs were carefully removed and cleaned ultrasonically in 96% ethanol (Otto Fischar GmbH) for 5 min (Sonorex Super RK1022, Bandelin). Specimens were then post-cured for 10 min in the LC-3DPrint Box (NextDent, Soesterberg, The Netherlands) according to the manufacturer’s specifications. The Dental LT Clear V2 resin met the ISO 7405:2018 biocompatibility requirements and the ISO 10993-1:2018 biological assessment standards for medical devices, making it suitable for clinical light-curing 3D printing.
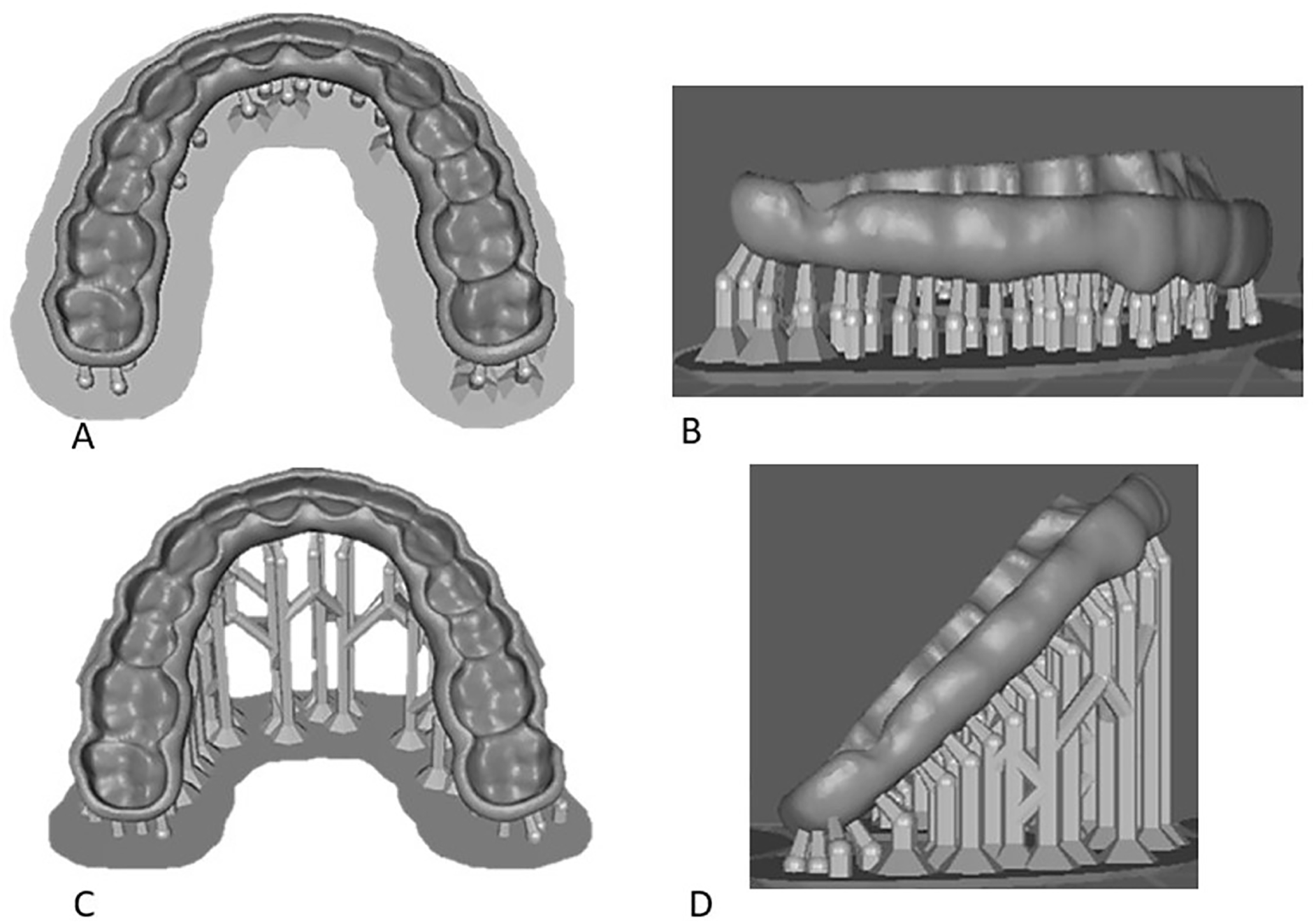
Figure 2. Images of designed occlusal devices. (A) Top view of 0° orientation; (B) Lateral view of 0° orientation; (C) Top view of 45° orientation; (D) Lateral view of 45° orientation
The OC’s surface roughness was measured using a Surtronic profilometer (Taylor Hobson) prior to delivery. To assess occlusal wear and obtain an STL file, OCs were digitized at baseline and after six months of use with a high-resolution scanner with 0.03 mm sensitivity (Solutionix, Solutionix Inc.) An experienced CAD investigator performed superimpositions at 24 predefined points to evaluate occlusal wear: 16 posterior (buccal/palatal cusps of maxillary molars/premolars) and 8 anterior (incisal edges of canines/lateral incisors, plus 2 palatal points at the maxillary canines). Geomagic Control X (3D Software System) was used to analyse all STL files. Following initial alignment, models were best-fit aligned in the buccal area (100% sampling, 500 iterations). A 3D analysis was conducted, generating a color map showing deviations within a 1.0 mm range between the test and reference models. Occlusal wear was then quantified by analyzing depth and volume loss at the points mentioned before and wear loss recorded in μm.
Clinical efficacy was evaluated through the administration of the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) Axis I form at baseline and after six months of treatment. The evaluation included assessments of pain during mandibular movements, muscle tenderness, joint sounds, and the location and duration of facial and cranial pain. Pain levels were recorded by a Visual Analog Scale (VAS), ranging from 0 (no pain) to 100 (maximum pain), at both time points.
IBM SPSS Statistics version 26.0 (IBM Corp) was used, and a one-way ANOVA was conducted to compare the primary groups. The Kruskal-Wallis H test and post hoc analyses were utilised for non-parametric data. Qualitative data were analysed using the chi-squared test (α = 0.05).
Forty participants (average age 42 ± 2 years; 30% male, 70% female) were monitored over a period of 6 months. No adverse effects were noted. Adherence to the intervention protocol was documented. Statistical analyses were conducted using SPSS version 26, employing paired t-tests for continuous variables and chi-squared tests for categorical variables (p < 0.05). The principal outcome was the alteration in well-being score from baseline to 6 months. Secondary outcomes encompassed changes in satisfaction scores and adherence rates.
3.1. Surface roughness results between the groups
Table 1 and Figure 3 present the mean ± standard deviation values of surface roughness (Ra) for the groups. OC printing orientations were selected based on prior literature and clinical goals [9]. The 0-degree orientation, chosen for its shorter print time (due to fewer layers) and improved accuracy and surface properties, has been previously established [14,15]. The CPMMA group exhibited the highest surface roughness, at 0.070 ± 0.006 mm. However, MPMMA, 3D 0°, and 3D 45° groups demonstrated the following results, respectively: 0.048 ± 0.005, 0.063 ± 0.003, and 0.067 ± 0.004. No significant difference in surface roughness was observed between the CPMMA and 3D 45° groups. The difference in surface roughness was significant across all other study groups, except between these two. (p < 0.001) (Table 1). Both null hypotheses were partially accepted, showing that printing orientation does not affect the accuracy of SLA-printed occlusal devices, and that 3D-printed occlusal devices are not inferior to traditional devices in therapeutic effects, clinical performance (surface roughness, wear, antagonist tooth abrasion, device fit), or patient satisfaction. Surface roughness of interim restorations is critical for periodontal health. Roughness exceeding 0.2 μm promotes bacterial colonization, with 10 μm being the clinically acceptable limit [16,17]. In this study, coated materials exhibited Ra values between 0.038 μm and 0.087 μm, all of which were below this threshold. Conventional PMMA showed greater surface roughness than 3D-printed resins, likely due to compositional differences, a finding supported by previous research [18] and the work of Rizzante et al. [19]. This reinforces that material composition influences surface roughness.
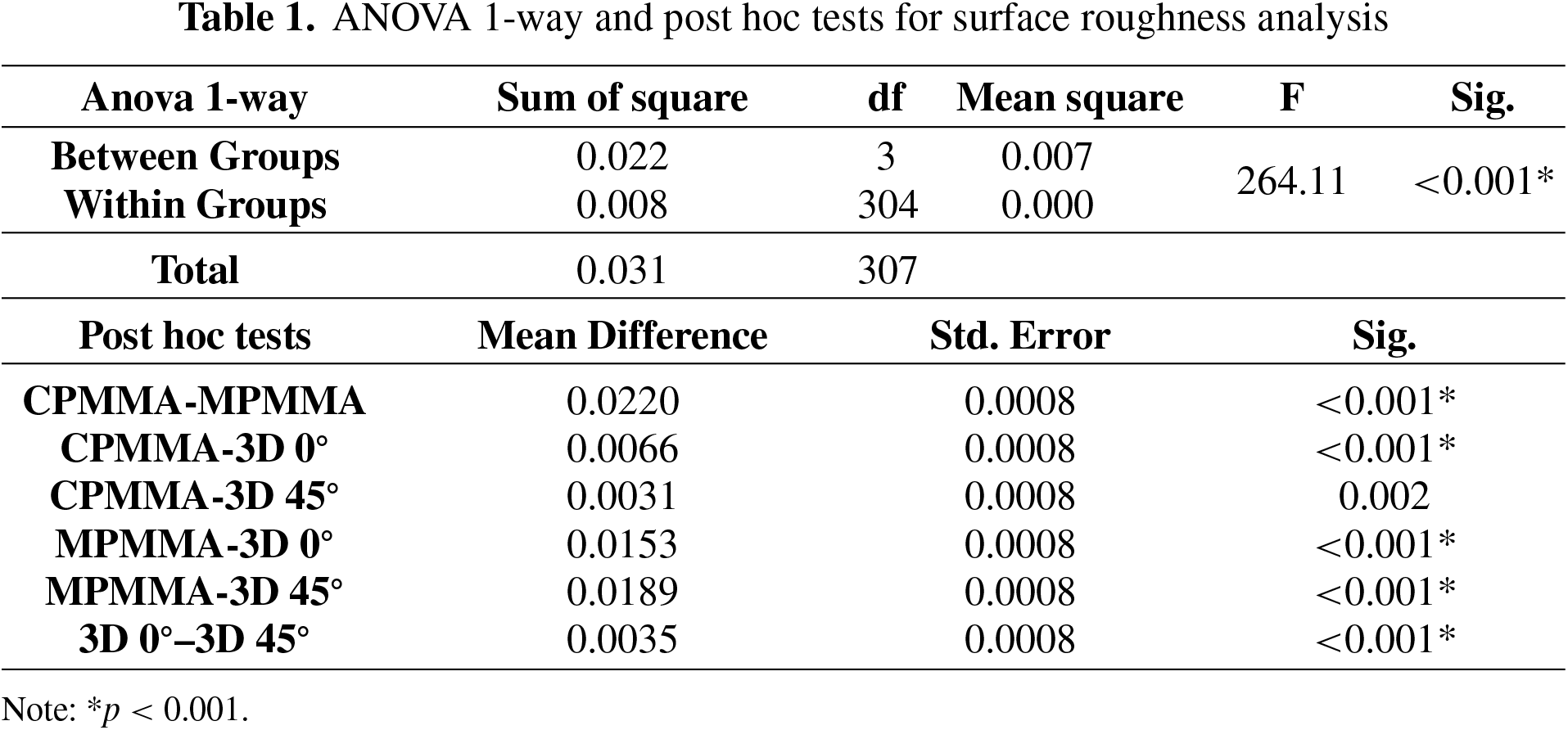

Figure 3. Surface roughness (Ra) values among tested subgroups
3.2. Surface wear results between the groups
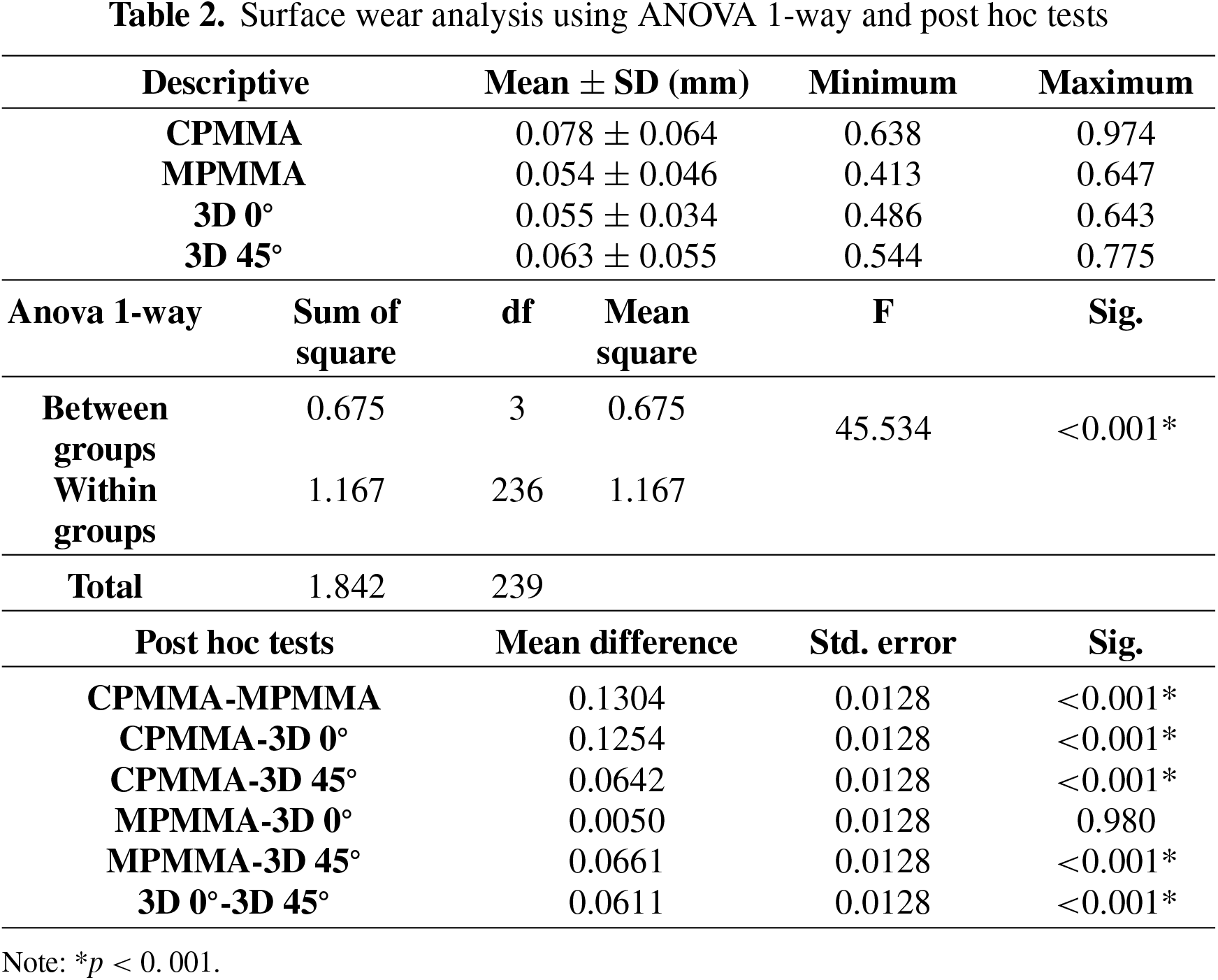
The mean ± standard deviation values of surface wear for the study groups were detailed in Table 2. The CPMMA group demonstrated the highest surface wear value of 0.078 ± 0.64 mm. No significant difference in surface wear was observed between the MPMMA and 3D 0° groups. The difference in surface wear was found to be significant among all other study groups except these two groups. (p < 0.001) (Table 2). Anisotropy, a directional dependence of material properties inherent in additive manufacturing due to its layer-by-layer process, significantly affects the mechanical behavior of 3D-printed polymers [20]. Studies investigating occlusal devices reveal variations in wear resistance, accuracy, and fit related to build orientation and layer thickness [21,22]. While some researchers have confirmed anisotropic behavior in 3D-printed OC [21], others found no significant differences across orientations [1]. The interlayer adhesion is a crucial factor influencing anisotropy, potentially explaining observed variations in mechanical performance across different build orientations. Studies indicate that the mechanical properties of 3D-printed resins are anisotropic [9,14]. For example, more vertically printed restorations show higher compressive strength and occlusal devices exhibit greater fracture resistance when printed vertically [14]. Consequently, the build direction should be chosen based on the desired mechanical property and manufacturer guidelines. The analysis of surface wear revealed a significant difference between the 3D printed groups and the control group, with the former showing a statistically significant reduction in wear. This finding is noteworthy, particularly because the participants had temporomandibular joint disorder (TMD), known for exerting substantial bite forces. Despite these elevated forces, the 3D printed materials exhibited superior wear resistance compared to the control group. Thus, the data strongly supports the enhanced performance of 3D printed materials regarding wear resistance under the challenging conditions associated with TMD.
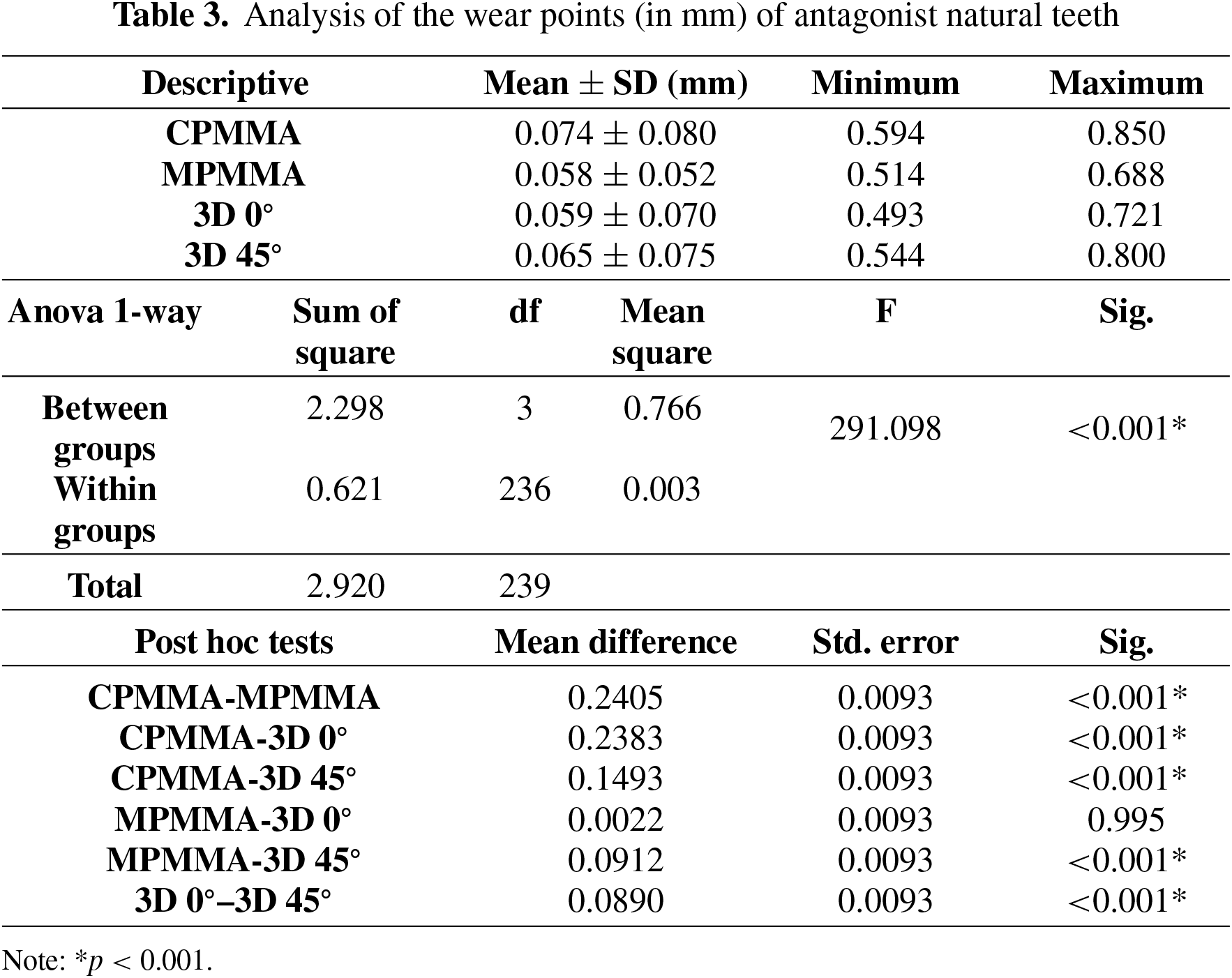
3.3. Surface wear results in antagonist natural teeth
Table 3 presents the mean ± standard deviation values of surface wear results in antagonist natural teeth after 6 months of treatment. Significant differences in antagonist tooth wear (p < 0.001) were observed between the control group and the study groups (Table 3). The degree of surface wear observed on natural antagonist teeth was statistically similar between the MPMMA and 3D 0° groups. Printing orientation significantly affected the amount of antagonist tooth wear. The 3D 0° group exhibited statistically significantly less wear on opposing teeth than the 3D 45° group, indicating that printing orientation influences abrasive wear. Notably, the 3D 0° group consistently exhibited the lowest wear levels throughout the study.
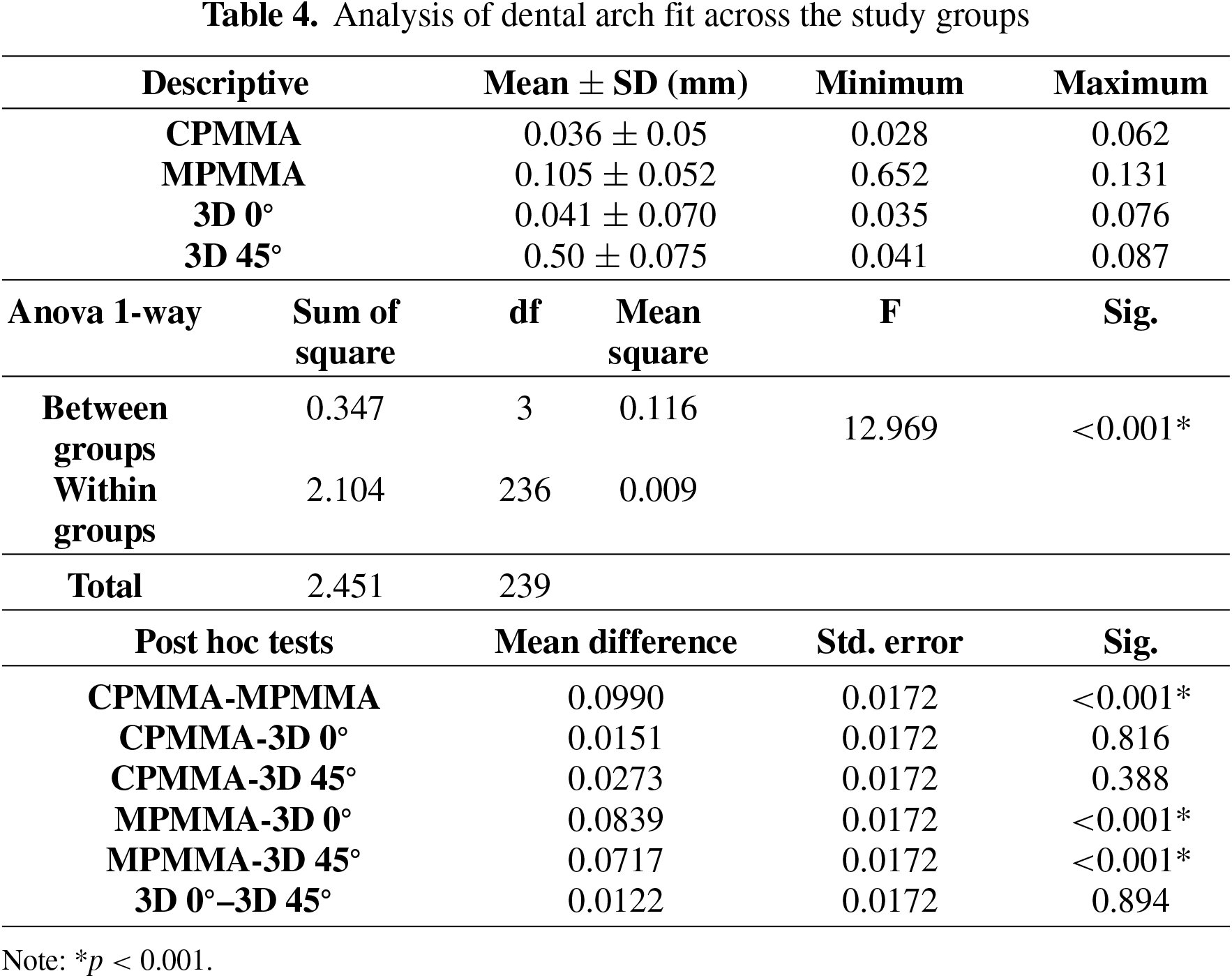
3.4. Analysis of dental arch fit across the study groups
Table 4 represents that the MPMMA group exhibited superior dental arch fit (0.058 ± 0.052) and minimal deviation compared to the study groups (p < 0.001). Both printed groups did not differ significantly from the control group. Furthermore, the groups produced with the 3D printer did not differ from one another in the best-fit evaluation. Reymus et al. [15] investigated the effect of print layer thickness on dimensional accuracy and related to fit accuracy, revealing that layers of 50 μm and 100 μm yield better precision than a 25 μm layer. They hypothesized that the enhanced light penetration of the thinner layer may cause over-curing, which could distort the final dimensions, as noted in the reference. Based on these findings and manufacturer recommendations, the present study selected a 100 μm layer thickness to optimize compatibility with the printing process and enhance fit accuracy. Unlike previous studies, this research found no statistically significant correlation between printed OC angle orientation and fit accuracy [11]. Consequently, future optimisation efforts could explore other factors influencing fit, including print resolution, material properties, support structure density, and curing protocol. Further investigation into these areas could enhance the precision and reliability of printed parts for applications demanding tight tolerances. Printing at a 0-degree orientation minimizes print time and maximizes accuracy due to the reduced number of layers [9]. In contrast, higher angles (60 degrees and above) increase print time because of the greater number of Z-axis layers, although they allow for more efficient use of the build plate, which may compromise accuracy [6,9]. Previous studies have shown that SLA-printed OC exhibit decreased accuracy and precision as the build orientation increases [23]. Specifically, researchers found that OC created with building angles below 60 degrees yielded higher accuracy compared to those produced at higher angles [23]. This current study focuses on a 45-degree orientation [9], which may enhance mechanical properties by optimizing the interaction between load direction and layer bonding [24]. This angle also allows for denser packing of OC compared to a 0-degree orientation. Earlier research suggests that a 45-degree orientation can contribute significantly to the mechanical properties of printed objects, highlighting the importance of load direction and layer bonding [24]. In our findings, the 0-degree orientation exhibited superior accuracy and fit for the OC groups compared to the 45-degree configuration. This improvement can be attributed to the alignment of print layers with the primary load-bearing directions, which minimizes interlayer defects and enhances dimensional stability. On the other hand, the 45-degree orientation introduces additional interlayer interfaces that may compromise the tightness and fit of the OCs. Anisotropic properties lead to orientation-dependent mechanical characteristics; therefore, 0-degree builds enhance stiffness and surface finish along the critical fit axis. Despite the potential for faster print times, the observed accuracy benefits suggest that minimizing layer interfaces with 0-degree builds outweighs the time savings for these occlusal devices.
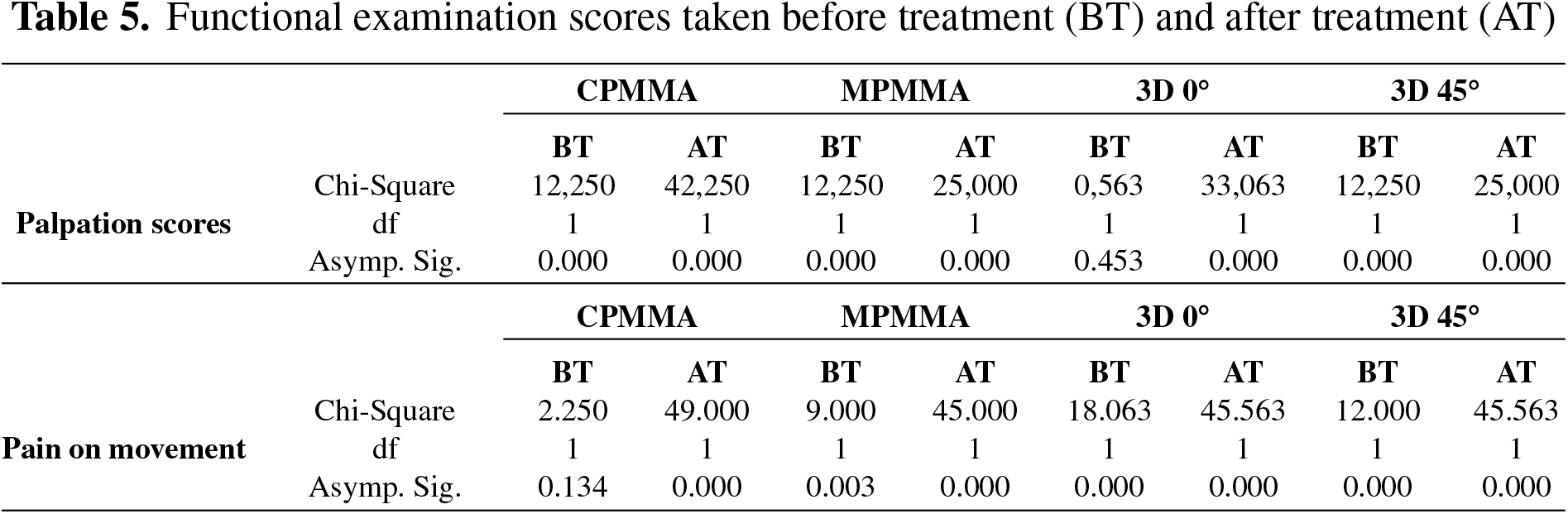
3.5. Therapeutic effects cores before treatment (BT) and after treatment (AT)
The chi-squared analysis results in Table 5 showed statistically significant improvements in the treatment group across all categories. Specifically, the treatment intervention led to a substantial and statistically significant reduction in reported pain during palpation, as well as a marked and statistically significant improvement in mandibular movement capabilities (p < 0.001). These findings indicate an overall improvement in jaw function following treatment. Furthermore, the analysis revealed that pain during movement also significantly decreased after treatment. This observed decrease in pain during movement was consistent across all groups assessed, with the statistical significance reaching a high level (p < 0.001). The consistent and statistically significant reductions in both palpation-induced and movement-related pain, coupled with improved mandibular movement, strongly suggest the treatment’s effectiveness in improving jaw function and reducing pain. The preceding clinical investigation, as outlined in reference [25], utilized a follow-up period of three months, during which outcome assessments were based on observations conducted at the end of this designated timeframe. In contrast to this earlier methodology, the present study proposes that 3D-printed occlusal devices, in conjunction with conventional CAD-CAM fabricated appliances, can be utilized with a credible expectation of safety for an extended duration of up to six months, without inducing adverse complications.
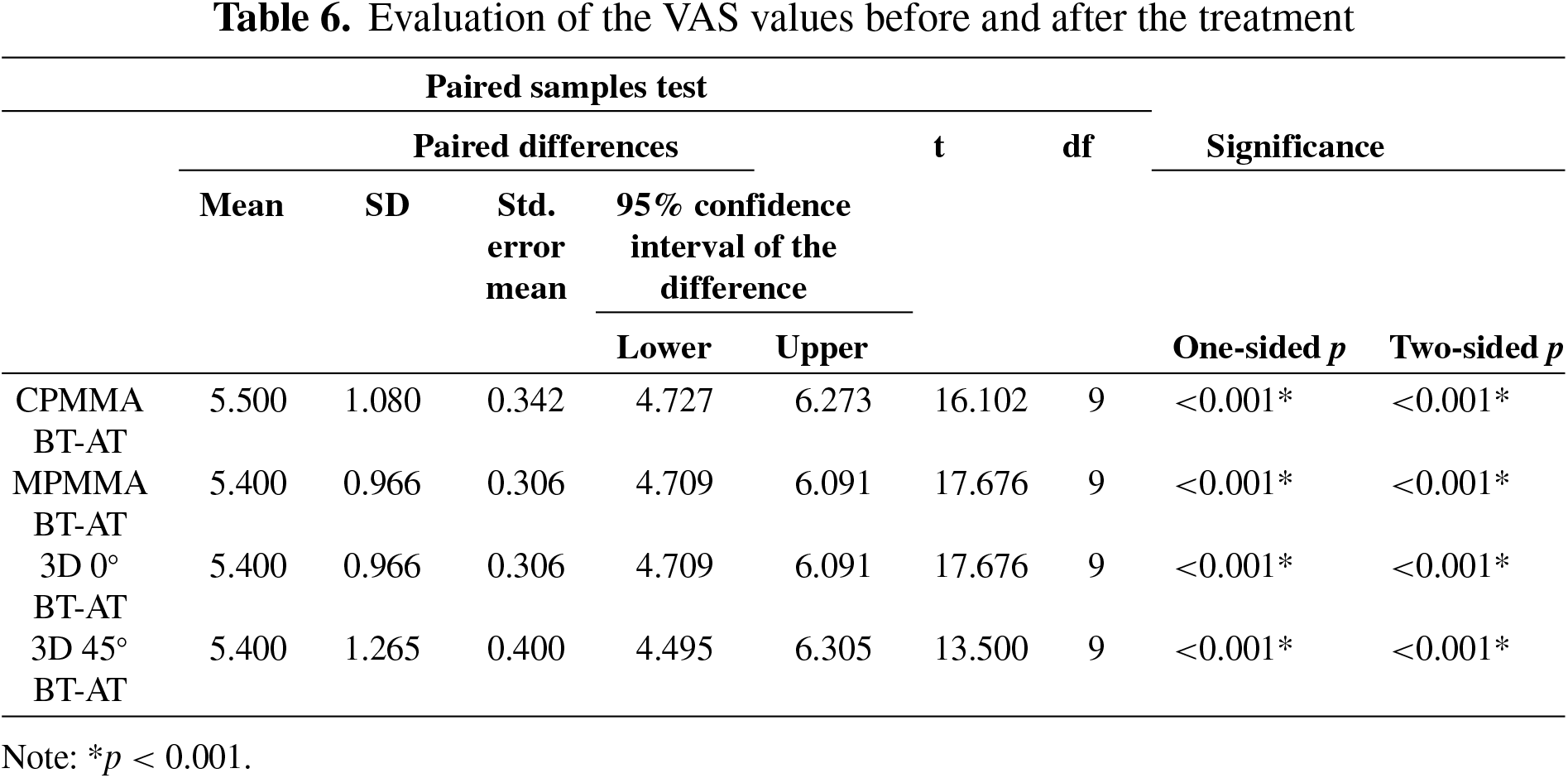
3.6. Assessment of visual analog scale (VAS) scores before and after treatment
The analysis of participant-reported pain, measured using a Visual Analog Scale (VAS), demonstrated a statistically significant reduction in pain across all treatment groups following the intervention (p < 0.001). However, comparisons between groups revealed no statistically significant difference in pain reduction (p < 0.001; Table 6), indicating similar pain-relieving effects across all treatment methods. These findings suggest that 3D-printed OCs offer pain relief comparable to conventional treatments and can therefore be considered a valid and effective method of pain management. Previous studies found no link between participant satisfaction and the manufacturing technique [26,27]. In this study, participants evaluated their pain but were not asked about the comfort or ease of use of the occlusal devices. No additional feedback regarding patient satisfaction was collected. Future research should incorporate patient satisfaction into its assessments and explore alternatives, such as modified, thinner, lighter occlusal devices or different colour variations, to enhance patient comfort.
The limitation of using a single resin type is that variations in viscosity and curing properties across resins and manufacturers can affect results. Therefore, it is important to interpret results while considering the specific resin, printing parameters, printer, software, and analysis methods used; this prevents broad generalizations. Assessing the accuracy of 3D-printed OC is limited by resin selection, inconsistent measurement methods, and software variations. Standardized protocols for materials and measurement are needed for reliable assessments. Optimizing printing involves balancing performance with cost and time. This study didn’t examine the time/cost of layer thickness or post-processing, nor did it assess water absorption, fatigue resistance, or bacterial adhesion, all vital for clinical outcomes. Future research should compare printers and different types of resins, evaluate printing orientations’ impact, and clinically assess 3D-printed OC to improve surface finish, durability with a larger number of participants, and interlayer bonding.
Advances in digital technologies enable new occlusal device materials and production methods, requiring mechanical evaluation under bruxism. This study investigated the six-month clinical effects of 3D-printed occlusal devices—printing orientation, therapeutic outcomes, clinical performance (surface roughness, wear, antagonist tooth abrasion, device fit), and patient satisfaction—in patients. Material and printing orientation significantly affected surface texture; conventional PMMA had the roughest surface and greatest wear, while milled PMMA and 3D-printed PMMA were smoother. Among 3D-printed options, wear resistance improved, particularly in the orientation matching milled PMMA performance. After six months, antagonist tooth wear was highest in the control group and lowest at 0° orientation, demonstrating the importance of load direction. The 0° orientation consistently yielded the lowest wear, suggesting its suitability for patients with high occlusal loads. It is crucial to understand and mitigate anisotropy to optimize OC design, as these devices must endure functional loads while maintaining dimensional accuracy in clinical conditions.
Milled PMMA provided the best arch fit; 3D-printed groups showed comparable fits to the control group. All modalities offered therapeutic benefits, reducing pain and improving mandibular movement similarly, supporting the clinical viability of 3D-printed devices for TMD-related pain management. Material selection and printing orientation significantly impacted surface properties and clinical performance. Clinically, all treatments achieved comparable pain relief and improved function, indicating that 3D-printed occlusal devices are a viable alternative to conventional methods with appropriate printing parameters and post-processing. Future research should optimize print settings and assess long-term outcomes. Overall, 3D-printed occlusal devices performed as expected and are suitable for their intended use, offering a potentially effective treatment option with favorable mechanical characteristics. Nevertheless, further investigations involving a larger number of participants are necessary to substantiate and reinforce the conclusions drawn from the current research.
Acknowledgement: Not applicable.
Funding Statement: This project was supported by the Research Universities Support Program (ADEP) with project number TSA-2024-40536.
Author Contributions: The authors confirm contribution to the paper as follows: study conception and design: Deger Ongul; data collection, analysis and interpretation of results: Bilge Gokcen-Rohlig; draft manuscript preparation: Deger Ongul. All authors reviewed and approved the final version of the manuscript.
Availability of Data and Materials: The data that support the findings of this study are available from the Corresponding Author, [Deger Ongul], upon reasonable request.
Ethics Approval: Ethical batch number TDK 2024/35910.
Conflicts of Interest: The authors declare no conflicts of interest.
Abbreviations
| OD | Occlusal devices |
| 3D | 3 Dimensional |
| AM | Additive manufacturing |
| SLA | Stereolithography |
| PMMA | Polymethyl methacrylate |
| CAD | Computer-Aided Design |
| CAM | Computer-Aided Manufacturing |
| TMD | Temporomandibular disorders |
| VA | Visual analog scale |
How to Cite this Article
References
- van Lingen C, Tribst JPM. 3D-printed occlusal splints: a narrative literature review. J Adv Oral Res. 2025;16(1):25–33. doi:10.1177/23202068251317825. DOI
- Alqarawi FK. The influence of printing orientation on the properties of 3D-printed polymeric provisional dental restorations: a systematic review and meta-analysis. J Funct Biomater. 2025;16(8):278. doi:10.3390/jfb16080278; 40863298 DOI
- Alharbi N, Wismeijer D, Osman R. Additive manufacturing techniques in prosthodontics: where do we currently stand? a critical review. Int J Prosthodont. 2017;30(5):474–84. doi:10.11607/ijp.5079; 28750105 DOI
- Revilla-León M, Özcan M. Additive manufacturing technologies used for processing polymers: current status and potential application in prosthetic dentistry. J Prosthodont. 2019;28(2):146–58. doi:10.1111/jopr.12801; 29682823 DOI
- Al Rashid A, Ahmed W, Khalid MY, Koç M. Vat photopolymerization of polymers and polymer composites: processes and applications. Addit Manuf. 2021;47(80):102279. doi:10.1016/j.addma.2021.102279. DOI
- Reymus M, Fabritius R, Keßler A, Hickel R, Edelhoff D, Stawarczyk B. Fracture load of 3D-printed fixed dental prostheses compared with milled and conventionally fabricated ones: the impact of resin material, build direction, post-curing, and artificial aging—an in vitro study. Clin Oral Investig. 2020;24(2):701–10. doi:10.1007/s00784-019-02952-7; 31127429 DOI
- Orgev A, Levon JA, Chu TG, Morton D, Lin WS. The effects of manufacturing technologies on the surface accuracy of CAD-CAM occlusal splints. J Prosthodont. 2023;32(8):697–705. doi:10.1111/jopr.13610; 36227731 DOI
- Revilla-León M, Cascos-Sánchez R, Zeitler JM, Barmak AB, Kois JC, Gómez-Polo M. Influence of print orientation and wet-dry storage time on the intaglio accuracy of additively manufactured occlusal devices. J Prosthet Dent. 2024;131(6):1226–34. doi:10.1016/j.prosdent.2022.12.005; 36635137 DOI
- de Castro EF, Nima G, Rueggeberg FA, Araújo-Neto VG, Faraoni JJ, Palma-Dibb RG, et al. Effect of build orientation in gloss, roughness and color of 3D-printed resins for provisional indirect restorations. Dent Mater. 2023;39(7):e1–11. doi:10.1016/j.dental.2023.05.002; 37248138 DOI
- Vasques MT, Laganá DC. Accuracy and Internal Fit of 3D printed Occlusal Splint, according to the printing position: a technique report. Clin Lab Res Dent. 2018:1–6. doi:10.11606/issn.2357-8041.clrd.2018.148012. DOI
- Cruz-Araújo SR, Sampaio-Fernandes MA, de Freitas BN, Simionato AA, Figueiral MH, Macedo AP. Accuracy of occlusal splints printed in different orientations by liquid crystal display technology: an in vitro study. J Dent. 2025;152:105461. doi:10.1016/j.jdent.2024.105461; 39542078 DOI
- Ohrbach R, editor editor. Diagnostic criteria for temporomandibular disorders: assessment instruments [Internet]. [cited 2026 Jan 1]. Available from: https://inform-iadr.com/wp-content/uploads/2024/08/DC-TMD-Thai-Assessment-Instruments_2023_01_27.pdf.
- Pecenek D, Gokcen-Rohlig B, Ongul D, Ayvalioglu DC. Evaluation of the clinical performance of different occlusal device materials. J Prosthet Dent. 2025;134(5):1806–12. doi:10.1016/j.prosdent.2024.04.021; 38806342 DOI
- Väyrynen VOE, Tanner J, Vallittu PK. The anisotropicity of the flexural properties of an occlusal device material processed by stereolithography. J Prosthet Dent. 2016;116(5):811–7. doi:10.1016/j.prosdent.2016.03.018; 27312654 DOI
- Reymus M, Lümkemann N, Stawarczyk B. 3D-printed material for temporary restorations: impact of print layer thickness and post-curing method on degree of conversion. Int J Comput Dent. 2019;22(3):231–7; 31463487
- Taşın S, Ismatullaev A, Usumez A. Comparison of surface roughness and color stainability of 3-dimensionally printed interim prosthodontic material with conventionally fabricated and CAD-CAM milled materials. J Prosthet Dent. 2022;128(5):1094–101. doi:10.1016/j.prosdent.2021.01.027. DOI
- Ozer NE, Sahin Z, Yikici C, Duyan S, Ali Kilicarslan M. Bacterial adhesion to composite resins produced by additive and subtractive manufacturing. Odontology. 2024;112(2):460–71. doi:10.1007/s10266-023-00862-5; 37819468 DOI
- Ribeiro AKC, de Freitas RFCP, de Carvalho IHG, de Miranda LM, da Silva NR, de Fátima D, et al. Flexural strength, surface roughness, micro-CT analysis, and microbiological adhesion of a 3D-printed temporary crown material. Clin Oral Investig. 2023;27(5):2207–20. doi:10.1007/s00784-023-04941-3; 36933047 DOI
- Rizante FAP, Bombonatti JSF, Vasconcelos L, Porto TS, Teich S, Mondelli RFL. Influence of resin-coating agents on the roughness and color of composite resins. J Prosthet Dent. 2019;122(3):332.e1–5. doi:10.1016/j.prosdent.2019.05.011; 31383532 DOI
- Zohdi N, Yang RC. Material anisotropy in additively manufactured polymers and polymer composites: a review. Polymers. 2021;13(19):3368. doi:10.3390/polym13193368; 34641184 DOI
- Wulff J, Rauch A, Schmidt MB, Rosentritt M. Biaxial flexural strength of printed splint materials. Materials. 2024;17(5):1112. doi:10.3390/ma17051112; 38473585 DOI
- Alqutaibi AY, Al-Gabri RS, Al-Zaghruri AS, Farghal AE, Alnazzawi AA, Alghauli MA. Clinical performance, accuracy, and physical-mechanical properties of 3D-printed removable partial denture metal frameworks compared with conventionally and partially digitally produced frameworks: a systematic review. J Prosthodont Res. 2026;70(2):206–23. doi:10.2186/jpr.jpr_d_25_00028; 40903281 DOI
- Saadat Sarmadi B, Schmidt F, Beuer F, Metin DS, Simeon P, Nicic R, et al. The effect of build angle and artificial aging on the accuracy of SLA- and DLP-printed occlusal devices. Polymers. 2024;16(12):1714. doi:10.3390/polym16121714; 38932064 DOI
- Unkovskiy A, Bui PH, Schille C, Geis-Gerstorfer J, Huettig F, Spintzyk S. Objects build orientation, positioning, and curing influence dimensional accuracy and flexural properties of stereolithographically printed resin. Dent Mater. 2018;34(12):e324–33. doi:10.1016/j.dental.2018.09.011; 30293688 DOI
- Al-Moraissi EA, Conti PCR, Alyahya A, Alkebsi K, Elsharkawy A, Christidis N. The hierarchy of different treatments for myogenous temporomandibular disorders: a systematic review and network meta-analysis of randomized clinical trials. Oral Maxillofac Surg. 2022;26(4):519–33. doi:10.1007/s10006-021-01009-y; 34674093 DOI
- Pho Duc JM, Hüning SV, Grossi ML. Parallel randomized controlled clinical trial in patients with temporomandibular disorders treated with a CAD/CAM versus a conventional stabilization splint. Int J Prosthodont. 2016;29(4):340–50. doi:10.11607/ijp.4711; 27479339 DOI
- Berntsen C, Kleven M, Heian M, Hjortsjö C. Clinical comparison of conventional and additive manufactured stabilization splints. Acta Biomater Odontol Scand. 2018;4(1):81–9. doi:10.1080/23337931.2018.1497491; 30128331 DOI