Abstract
Keywords: Bulk-fill composites; fiber-reinforced resin; flexural strength; degree of conversion; composite reparability
Dental composites are the cornerstone of modern restorative dentistry due to their superior aesthetics, handling properties, and clinical performance [1]. Among these, bulk-fill composites have gained considerable acceptance for their ability to be applied in large increments, thus reducing clinical chair time while maintaining adequate polymerization and mechanical strength [2,3].
Bulk-fill composites are generally classified by viscosity into flowable and high-consistency types [4]. Flowable composites such as SDR Plus exhibit low viscosity and superior adaptability, making them suitable for use as a base in deep cavities. Conversely, low- to medium-viscosity composites like Beautifil Bulk Flow contain greater filler loading and enhanced mechanical strength, rendering them appropriate for direct posterior restorations A newer class of fiber-reinforced bulk-fill composites, exemplified by EverX Posterior, incorporates short E-glass fibers that significantly improve flexural strength and crack resistance, particularly in stress-bearing areas [5]. Nevertheless, issues such as polymerization shrinkage, incomplete degree of conversion, progressive mechanical degradation, and challenges in effectively repairing fractured restorations continue to compromise clinical outcomes [6,7]. Consequently, factors such as mechanical properties, efficiency of polymerization, thermal stability, and repair flexural strength are essential for ensuring the long-term durability of bulk-fill composites [8].
In clinical practice, selecting an appropriate bulk-fill composite requires balancing factors including ease of placement, curing efficiency, mechanical robustness, and reparability [9]. Despite the growing use of fiber-reinforced composites, limited attention has been given to their flexural strength, thermal stability, and reparability relative to conventional bulk-fill materials. Most studies have focused on isolated properties such as polymerization depth or mechanical strength, with insufficient exploration of how these factors interact to influence long-term restoration durability [10–12]. Repairing fractured bulk-fill composites is particularly challenging, and there is no established consensus on the best clinical protocols, especially for fiber-reinforced varieties. Flowable composites such as Filtek™ Supreme Flowable Restorative have been suggested to improve the bond strength of repairs due to their low viscosity and favorable wetting properties. Nevertheless, the application of fibre-reinforced bulk-fill composites for repair is scarcely documented. Besides, the degree of conversion is a crucial factor affecting both polymerization efficiency and the final mechanical behavior [13]. Fiber inclusions in reinforced composites may cause light scattering, reducing the depth of cure and consequently lowering the degree of conversion and mechanical integrity [14].
Addressing these gaps, the present study aims to comprehensively compare the flexural strength, degree of conversion, and repair flexural strength of three bulk-fill composites: SDR Plus, Beautifil Bulk Flow, and EverX Posterior. The findings will inform material selection and repair strategies in clinical restorative dentistry. Therefore, this study aimed to evaluate the flexural strength to assess the performance in stress-bearing conditions. It further examined the degree of conversion using ATR-FTIR spectroscopy and investigated the repair flexural strength of Filtek™ Supreme Flowable Restorative compared to self-repair. It was hypothesized that no significant differences would exist among the study materials in terms of flexural strength, degree of conversion and repair flexural strength.
Before conducting this research, IRB approval was obtained from the Riyadh Elm University (FPGRP/2024/828/1155/1079). The study evaluated three bulk-fill composite materials: two conventional composites—SDR Plus (Dentsply, Sirona, USA) and Beautifil Bulk Flow (Shofu, Kyoto, Japan)—and one fiber-reinforced composite, i.e., EverX Posterior (GC Corporation, Tokyo, Japan). Additionally, Filtek™ Supreme Flowable Restorative (3M™ ESPE, Seefeld, Germany) was used for repair procedures. The sample size estimation was performed using G*Power software (ver. 3.1.9.4) for one-way analysis of variance (ANOVA), assuming an effect size (f) of 0.75, a significance level (α) of 0.05, and a power of 0.95. The analysis indicated that 10 specimens per group were sufficient to ensure adequate power for the primary group comparisons.
For each composite material, 10 cylindrical specimens (2 mm height × 5 mm diameter) and 10 bar-shaped specimens (25 mm × 2 mm × 2 mm) were fabricated using silicone molds. Material placement involved a single increment filled within the molds, covered with a transparent plastic sheet and a glass slide to ensure a flat surface. Polymerization was performed with a high-power halogen light-curing unit (1000 mW/cm2; Hilux 250, Benlioğlu Dental, Ankara, Turkey). The unit was radiometer-tested before use. The light tip delivered 400–500 nm blue emission for camphorquinone activation in direct, perpendicular contact with the specimen for 40 s per curing area. Bar-shaped specimens were cured in three sections, each exposed for 40 s.
After curing, specimens were polished with 4000-grit silicon carbide paper to achieve uniform thickness, which was verified with a digital micrometer. Only specimens free from voids and dimensional flaws were included.
2.3 Degree of conversion (Dc) assessment
The degree of conversion (Dc) was measured on cylindrical specimens after 24 h of polymerization using Attenuated Total Reflectance Fourier Transform Infrared (ATR-FTIR) spectroscopy (NICOLET iS5, Thermo Scientific, Massachusetts, USA). Spectra were recorded between 500 and 4000 cm−1, focusing on the aliphatic C=C peak at approximately 1638 cm−1 and the aromatic C–C peak at 1608 cm−1. The aromatic C=C band at 1608 cm−1 was used as an internal reference, validated for camphorquinone photoinitiator systems across all tested bulk-fill composites. Spectra were acquired at a resolution of 4 cm−1, scan speed of 0.7 cm/s with 32 scans averaged per spectrum.
2.4. Flexural strength testing
Before flexural strength testing, bar-shaped specimens underwent thermocycling (Model 1100, SD Mechatronik, Feldkirchen-Westerham, Germany) for 5000 cycles between 5°C and 55°C in distilled water baths containing 10 L each. The specimens were fully immersed and suspended centrally in the bath, avoiding contact with the container walls. Bath temperatures were monitored and calibrated using an external digital thermometer to ensure that target temperatures (5 ± 1°C and 55 ± 1°C) were consistently maintained throughout the cycling protocol. The dwell time and transfer time were 10 s in each bath. The three-point bending test was conducted following ISO 4049 standards using a universal testing machine (Instron Model 3369, Instron, Canton, MI, USA) equipped with a 5 kN load cell. Specimens were loaded at a crosshead speed of 1.0 mm/min, with a support span of 20 mm and a loading piston diameter of 2 mm. Flexural strength (σ = 3FL/2bd2) was automatically computed by Instron software. Specimen dimensions (25 × 2 × 2 mm) were verified (±0.1 mm tolerance) using digital micrometer; deviations led to exclusion.
2.5. Repair flexural strength testing
Following the initial fracture during flexural testing, bar-shaped specimens were realigned in the molds for repair. Specimens from each composite group were randomly allocated to either the self-repair group (repair with the same composite material) or the flowable-repair group using simple random assignment (n = 5 per subgroup). Flexural strength testing was performed by a single operator who was blinded to the repair material during mechanical testing. Fractured surfaces were etched with 35% phosphoric acid (Scotchbond Etchant Gel; 3M™ ESPE, St. Paul, MN, USA) for 30 s, rinsed, and dried, followed by application of a Scotchbond Universal adhesive (3M™ Oral Care, St. Paul, MN, USA). Half of the specimens from each group were repaired with the same composite material, while the remaining half were repaired using Filtek™ Supreme Flowable Restorative. Composite was applied to fill the fracture gap, adapted with a plastic strip and glass slide, and light-cured for 40 s. Repaired specimens were stored for 24 h before undergoing thermocycling identical to the initial protocol. Subsequently, repaired specimens were subjected to the same three-point bending test and flexural strength was calculated (Figure 1).
Figure 1. Repaired bar-shaped sample of EverX Posterior composite: (A) EverX Posterior repaired with the same material, and (B) EverX Posterior composite repaired with Filtek™ supreme flowable restorative
Fractured surfaces of repaired specimens were examined under a stereomicroscope at 20× magnification. Failures were classified per ISO 4049 as: adhesive (at repair-substrate interface), cohesive (within composite), or mixed (involving both interfaces).
Data for flexural strength and degree of conversion were analyzed using one-way ANOVA with Tukey’s post hoc tests to identify intergroup differences. Repair flexural strength data were analyzed using two-way ANOVA (composite type × repair material), followed by Tukey’s post-hoc tests for group comparisons. Statistical significance was set at p < 0.05.
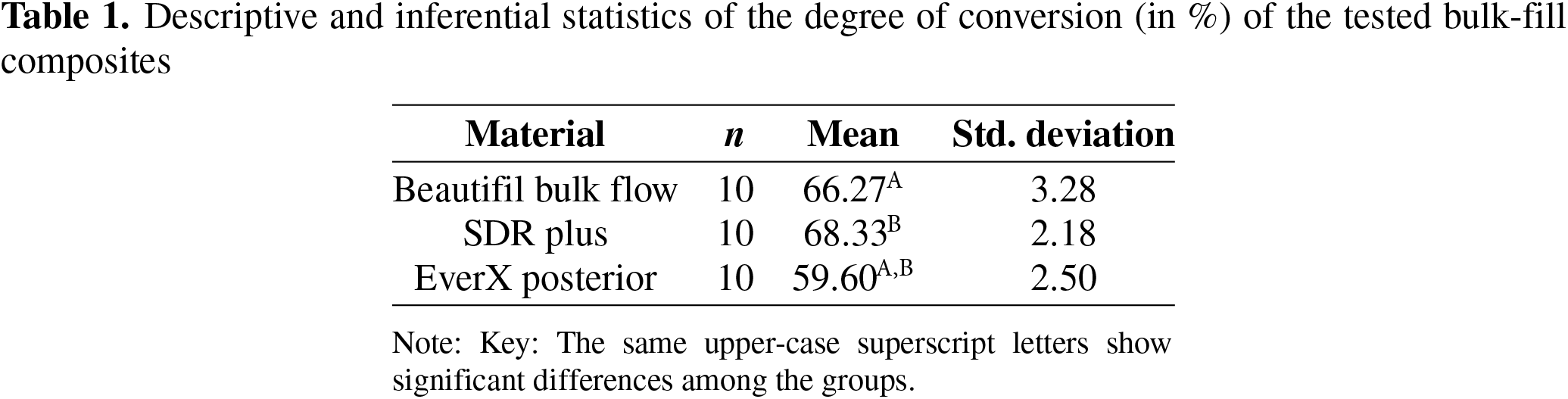
3.1. Degree of conversion (Dc)
The Dc findings are summarized in Table 1. SDR Plus exhibited the highest mean Dc (68.33% ± 2.18%), closely followed by Beautifil Bulk Flow (66.27% ± 3.28%). In contrast, the fiber-reinforced composite, EverX Posterior, demonstrated a significantly lower Dc (59.60% ± 2.50%). Statistical analysis by one-way ANOVA revealed a highly significant difference among the groups (F = 28.73, p < 0.001). Post-hoc comparisons confirmed that EverX Posterior differed significantly from both SDR Plus and Beautifil Bulk Flow (p < 0.001), while no significant difference was observed between SDR Plus and Beautifil Bulk Flow (p = 0.218).
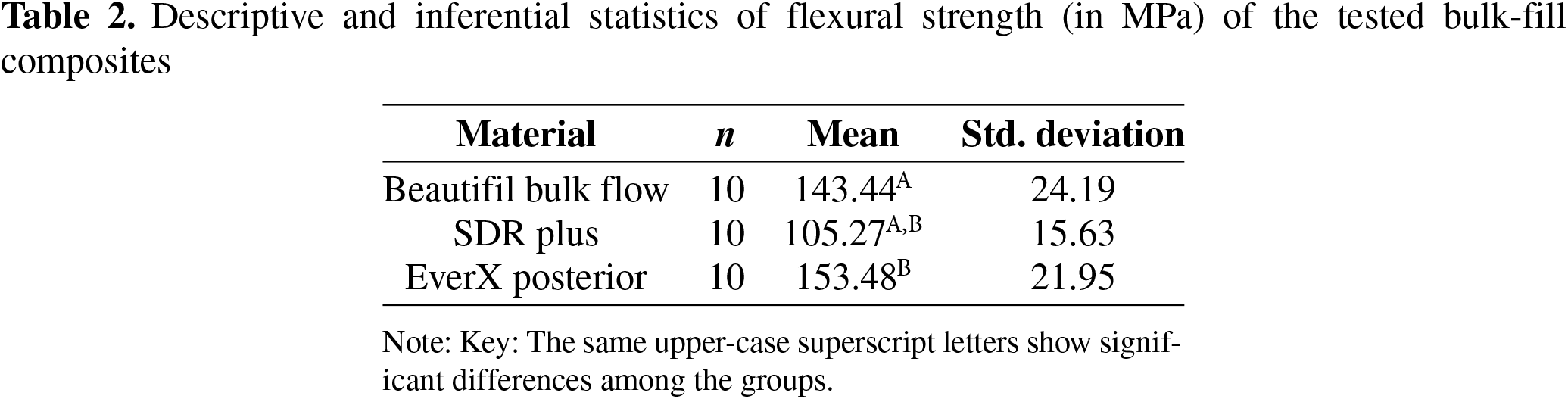
Descriptive data for flexural strength are presented in Table 2. EverX Posterior demonstrated the highest mean flexural strength (153.48 MPa ± 21.95), followed by Beautifil Bulk Flow (143.44 MPa ± 24.19), and SDR Plus showed the lowest values (105.27 MPa ± 15.63). One-way ANOVA indicated statistically significant differences among groups (F = 14.80, p < 0.001). Pairwise comparisons revealed that both EverX Posterior and Beautifil Bulk Flow had significantly higher flexural strength than SDR Plus (p = 0.001 and p < 0.001, respectively). In contrast, the difference between EverX Posterior and Beautifil Bulk Flow was not statistically significant (p = 0.538).
Repair flexural strength findings (Figure 2) indicated variable results depending on the repair material used. Beautifil Bulk Flow samples repaired with the same composite achieved a higher mean repair strength (87.86 MPa ± 34.43) than those repaired with the flowable composite (65.43 MPa ± 26.31). Conversely, SDR Plus exhibited slightly higher repair strength when repaired with flowable composite (87.59 MPa ± 12.94) compared to self-repair (80.74 MPa ± 22.83). Notably, EverX Posterior showed higher repair strength with flowable composite (94.13 ± 52.88 MPa) compared to self-repair (32.02 ± 34.16 MPa), though high variability was noted.
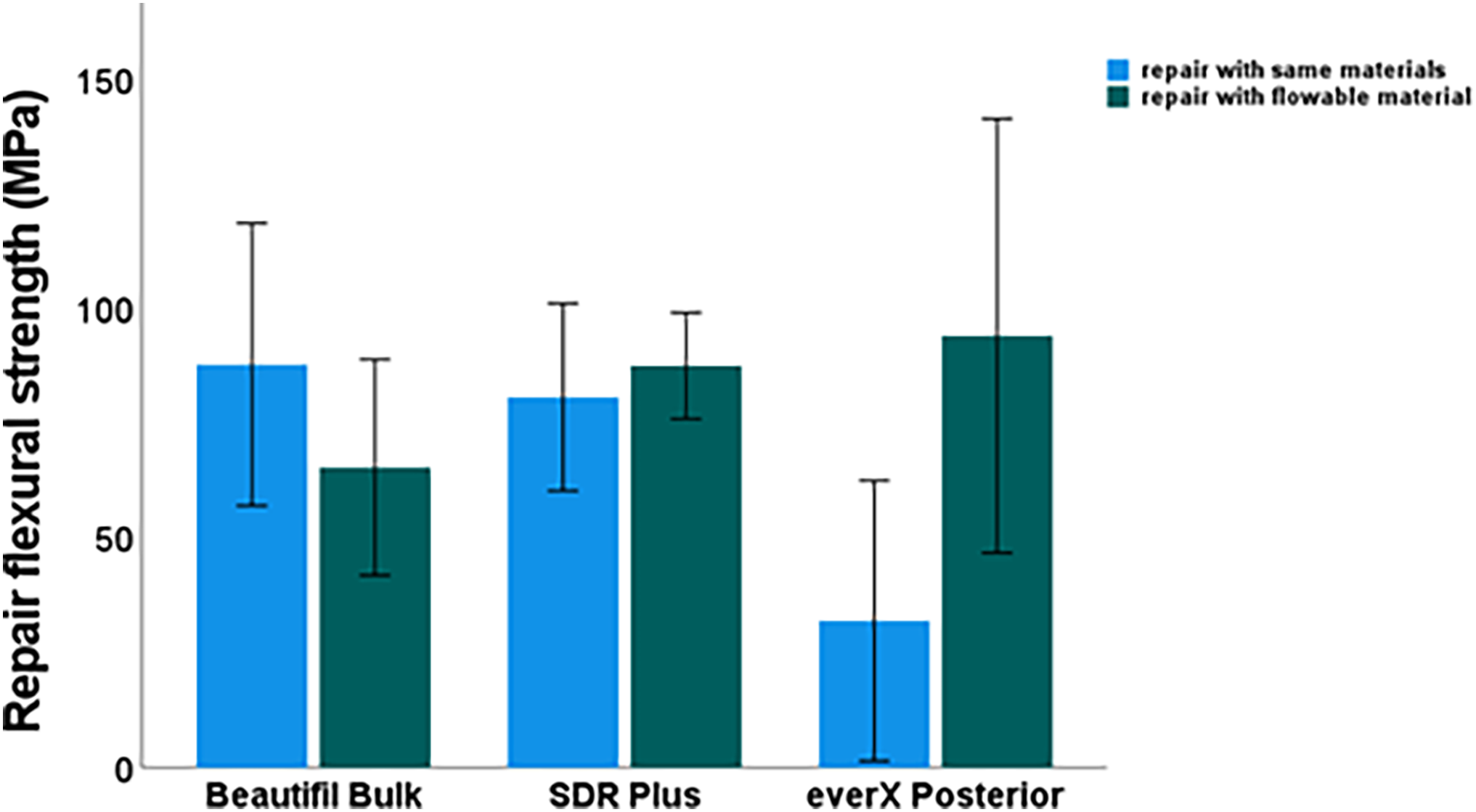
Figure 2. Comparison of repair flexural strength (MPa) of study composites repaired with the same materials vs. flowable composites. Error bars represent standard deviation
Two-way ANOVA revealed no significant main effects of repair material (p = 0.210) or composite type (p = 0.365), but a significant interaction between these factors (p = 0.027, partial η2 = 0.261). Therefore, simple-effects analyses were performed. No significant differences between repair methods were found for Beautifil Bulk Flow (p = 0.280) or SDR Plus (p = 0.576). For EverX Posterior, repair with flowable composite showed a trend toward higher repair flexural strength, although this difference did not reach statistical significance (p = 0.058).
When compared with the original specimens (Figure 3), all repaired groups exhibited lower flexural strength, highlighting that repair strategies, although beneficial, do not fully restore the strength of the bulk-fill composites.
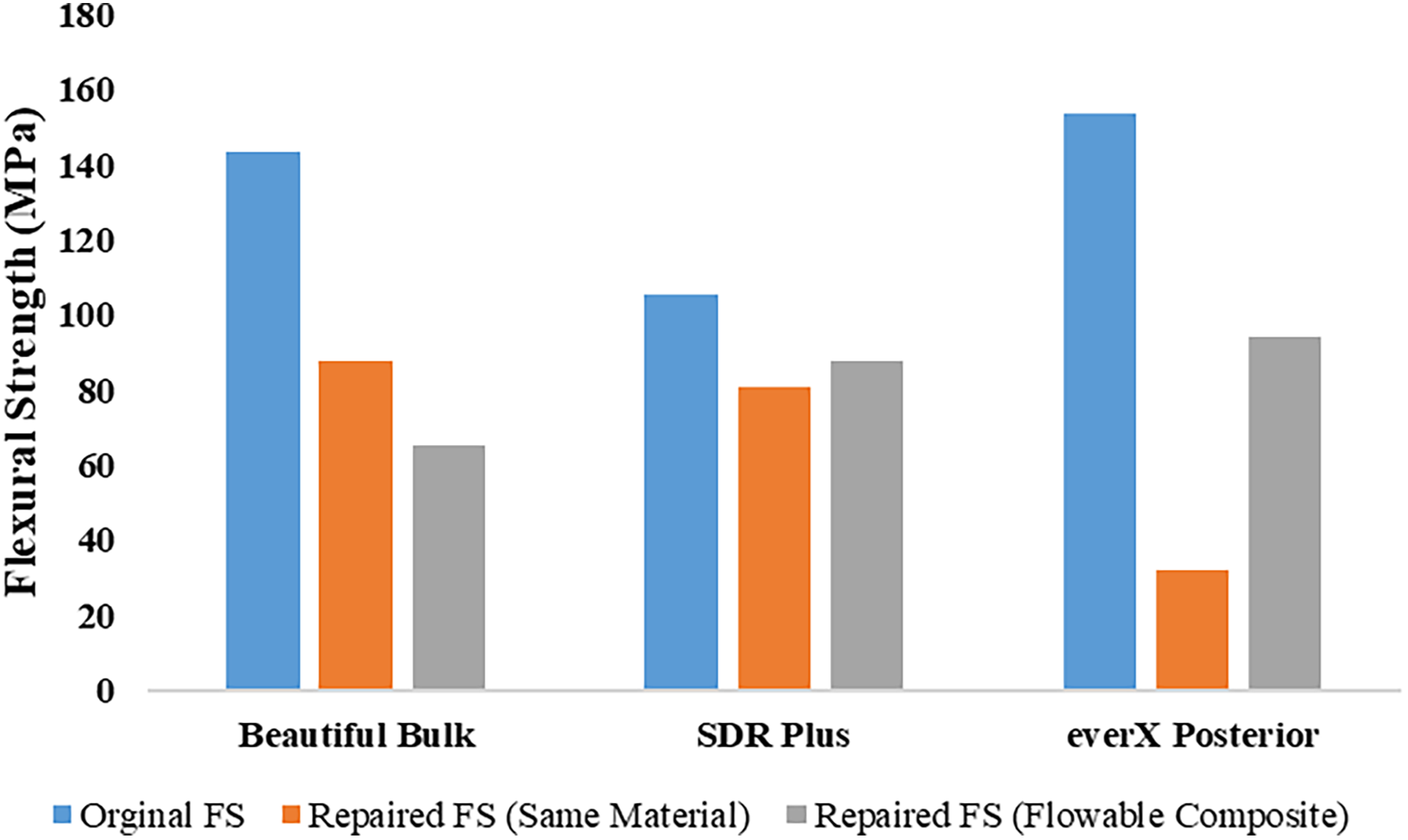
Figure 3. Comparison of flexural strength (MPa) among original specimens, specimens repaired with the same material, and specimens repaired with flowable composite across different bulk-fill composites
Failure mode evaluation (Table 3) revealed that adhesive failure was predominant across most groups. For Beautifil Bulk Flow, adhesive failures comprised 60% and 80% when repaired with the same composite and flowable composite, respectively, with no cohesive failures observed. SDR Plus showed a shift toward mixed failures (60%) when repaired with flowable composite, with 40% adhesive failures; no cohesive failures were detected. EverX Posterior demonstrated 20% cohesive failures exclusively in specimens repaired with the flowable composite, whereas specimens repaired with self-material exhibited 100% adhesive failures. Representative stereomicroscopic images supporting failure mode classifications are illustrated in Figures 4–6.
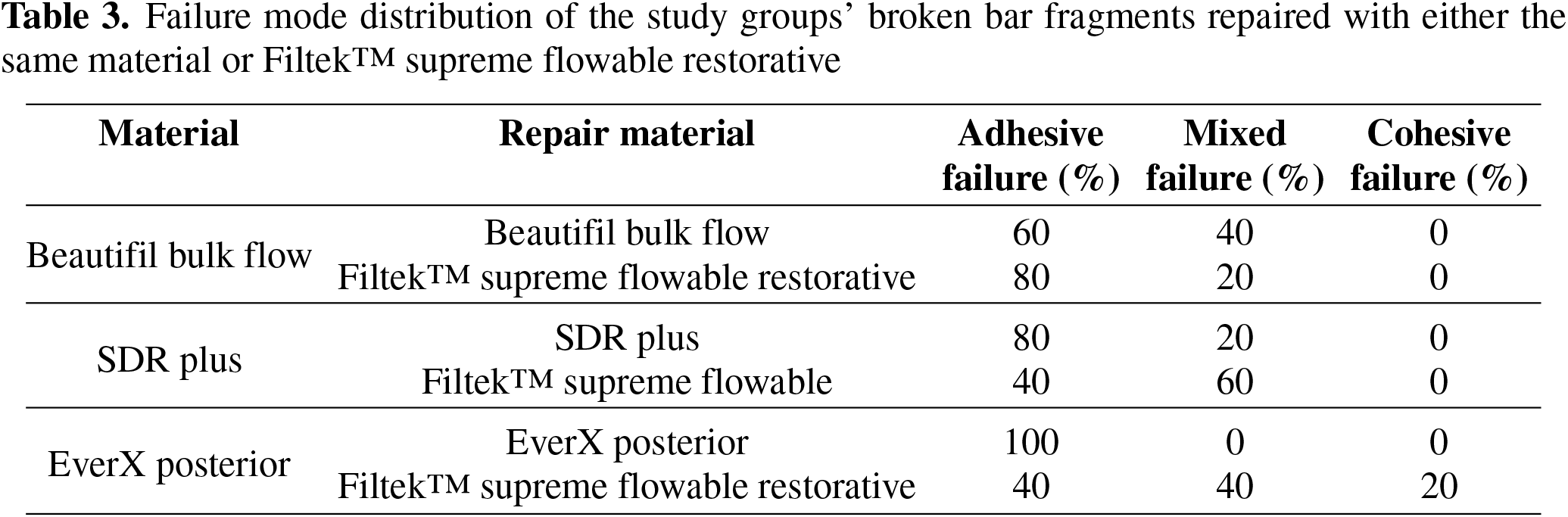
Figure 4. Representative images of repaired Beautifil Bulk Flow broken bar fragments: (A–C) Fragments repaired with the same material (Beautifil Bulk Flow) while (D–F): Fragments repaired with Filtek™ Supreme Flowable Restorative
Figure 5. Representative images of repaired SDRPlus broken bar fragments: (A–C) Fragments repaired with the same material (SDR Plus) while (D–F): Fragments repaired with Filtek™ supreme flowable restorative
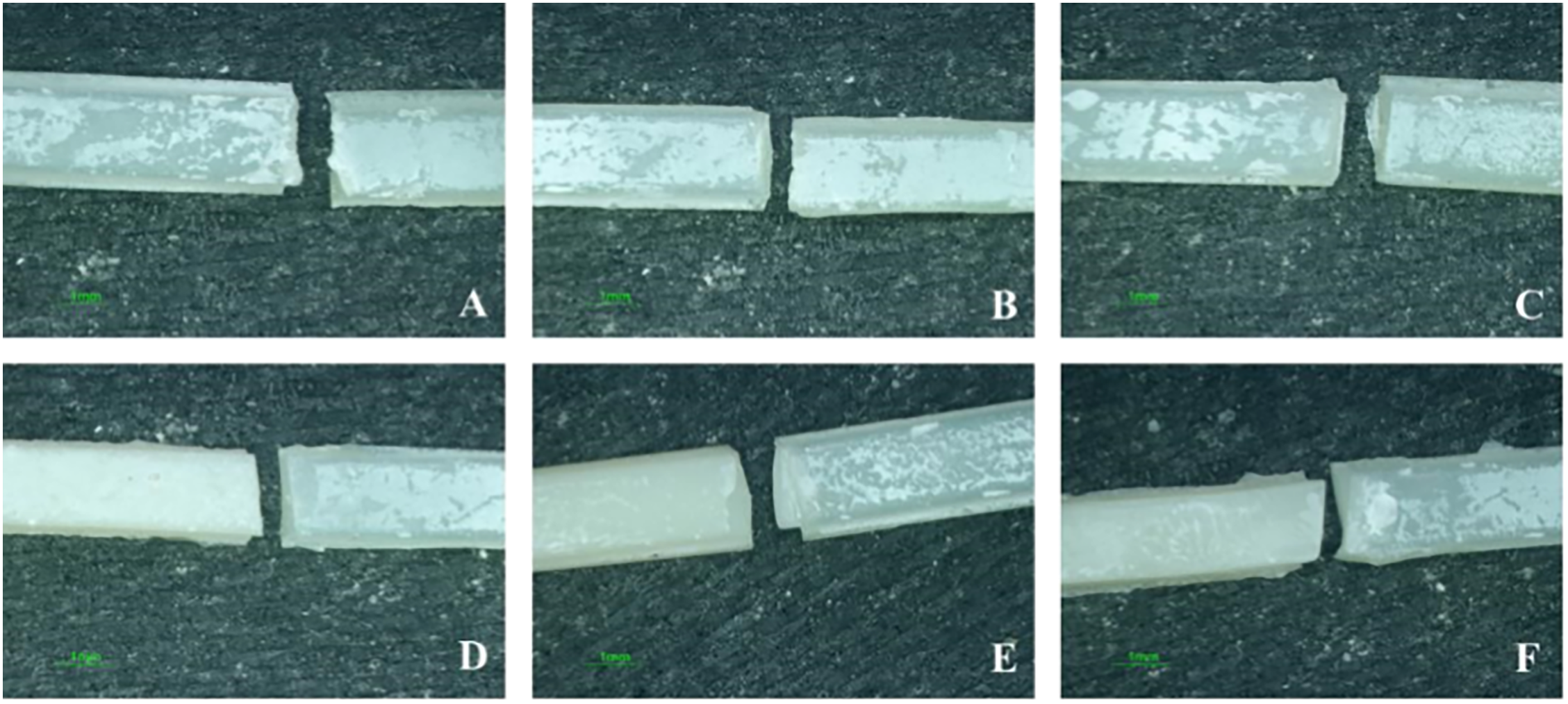
Figure 6. Representative images of repaired EverX Posterior broken bar fragments: (A–C) Fragments repaired with the same material (EverX Posterior), while (D–F): Fragments repaired with Filtek™ supreme flowable restorative
Of the three bulk-fill composites evaluated in this study, the fiber-reinforced EverX Posterior demonstrated superior mechanical properties and reparability, while the conventional composites SDR Plus and Beautifil Bulk Flow exhibited a higher Dc. Hence, the hypothesis that no significant differences would exist among the study materials in terms of flexural strength, degree of conversion and repair flexural strength is rejected.
Dc is a critical determinant of the mechanical properties and clinical performance of resin composites [15]. Analytical results indicated a significant disparity in Dc values among the materials tested: SDR Plus exhibited the highest Dc (68.33%), followed by Beautifil Bulk Flow (66.27%), while EverX Posterior demonstrated the lowest value (59.60%). The superior Dc of SDR Plus and Beautifil Bulk Flow is likely attributable to their higher translucency and lower filler content, which facilitates enhanced light transmission and more efficient polymerisation. SDR Plus, a flowable bulk-fill composite, is specifically designed to permit deeper light penetration, thereby promoting a higher degree of polymerization in bulk layers [16]. Although filled slightly more, Beautifil Bulk Flow incorporates highly translucent fillers that similarly contribute to its polymerization efficiency. Conversely, the reduced Dc of EverX Posterior is presumably a consequence of its fiber-reinforced composition. The incorporated fibers scatter and absorb light, thereby impeding the polymerization process, a finding consistent with the work of Alrahlah et al. [17]. The lower Dc of EverX Posterior is attributed to fiber light-scattering effects based on established literature; direct transmittance measurements were not performed and represent an avenue for future investigation. The present study used a halogen light-curing unit emitting primarily in the blue spectrum (400–500 nm), suitable for camphorquinone photoinitiators in the tested composites. While recent literature compares mono-wave and poly-wave LED curing [13], the halogen spectrum employed here effectively activated the primary photoinitiators, though future studies with poly-wave sources may further optimize bulk-fill performance.
These results suggest that SDR Plus and Beautifil Bulk Flow are more suitable for applications that require optimal polymerization. In contrast, EverX Posterior is better suited for high-stress-bearing applications where its exceptional mechanical properties are paramount, and the depth of cure is less critical.
Flexural strength is crucial in determining a material’s capability to endure forces that are exerted during mastication [18]. Of the materials tested, EverX Posterior demonstrated the highest flexural strength (153.48 MPa), followed by Beautifil Bulk Flow (143.44 MPa), with SDR Plus exhibiting the lowest value (105.27 MPa). This mechanical superiority of EverX Posterior is directly attributable to its fiber-reinforced composition, wherein the embedded fibers act to distribute occlusal loads and inhibit crack propagation [19,20]. This finding corroborates existing literature establishing the superior mechanical properties of fiber-reinforced composites over conventional and bulk-fill composites [10,11]. In contrast, the lower flexural strength values of Beautifil Bulk Flow and SDR Plus are consistent with their non-reinforced compositions. The particularly low strength of SDR Plus is characteristic of its flowable nature, which necessitates a lower filler load and a higher resin matrix fraction, resulting in reduced resistance to deformation [21]. Although Beautifil Bulk Flow possesses a higher filler content and greater strength than SDR Plus, its lack of fibrous reinforcement renders it more susceptible to fracture under high stress compared to the fiber-reinforced EverX Posterior [10].
We observed that repairing EverX Posterior with Filtek™ Supreme Flowable Restorative substantially increased bond strength (from 32.02 MPa in self-repair to 94.13 MPa with flowable repair), and showed higher values than SDR Plus and Beautifil Bulk Flow. However, the high standard deviations observed in the repair strength data indicate considerable variability and highlight the need for larger, preferably clinical, studies to confirm these findings. The higher repair flexural strength was achievable due to improved adhesion of flowable composite to EverX Posterior, based on the capability of monomers of universal adhesive and flowable composite to dissolve the semi-interpenetrating polymer network (IPN) of EverX Posterior [22]. EverX posterior contains a matrix system with both linear and cross-linked polymers. The solubility parameter of the monomer systems of the universal adhesive and flowable composite might be close to linear polymer used in EverX Posterior. Due to monomer diffusion in a linear polymer, a strong adhesive interface is formed [23]. Whereas the composition of both Beautifil Bulk Flow and SDR Plus does not contain semi-IPN. This lacks in monomer diffusion and eventually under flexural stress. The optimal bond achieved with fiber-reinforced composites aligns with previous findings that flowable composites penetrate micro-roughness efficiently, boosting repair outcomes [24,25].
Failure mode analysis provides insight into how composite materials fail under mechanical stress and upon repair [26]. SDR Plus exhibited predominantly adhesive failures, likely due to its lower filler content and higher polymerization shrinkage, leading to interfacial stress [27]. Beautifil Bulk Flow exhibited moderate bond strength and predominantly mixed failures, with a higher tendency toward cohesive fractures [28]. EverX Posterior demonstrated favorable failure modes with fewer cohesive failures when repaired using Filtek™ Supreme Flowable Restorative, attributed to fiber reinforcement that effectively transfers stress and limits crack propagation [29].
Clinically, these findings suggest that SDR Plus may be less suitable for load-bearing repairs due to adhesive failure risk and is better used as a base material. Beautifil Bulk Flow may need surface treatments like roughening or priming to improve repair bond strength. EverX Posterior provides superior repair outcomes for high-stress applications, especially when combined with flowable composites, supporting material selection and repair strategy decisions to enhance restoration durability.
Although this study offers valuable insights into mechanical performance, Dc and reparability of bulk-fill composites, its in vitro design does not replicate complex oral conditions such as salivary enzymes, biofilms, and occlusal forces. The thermocycling protocol simulated short-term aging but may not reflect long-term thermal stress. Besides, the lack of fatigue loading and bond strength tests (microtensile/shear) limits direct quantification of the repair interface. A key limitation was the omission of standard clinical steps, i.e., mechanical roughening and silanization, which are standard clinical procedures, particularly for glass fiber-containing composites. Future studies should test these pretreatment combinations. Future investigations should include long-term clinical trials to assess real intraoral behavior, exploration of advanced surface treatments to enhance repair bond strength, cyclic fatigue and wear resistance testing for realistic masticatory simulation. These directions will support evidence-based improvements in restorative dentistry.
This in vitro study demonstrates that fiber-reinforced EverX Posterior exhibited superior flexural strength but lower Dc compared to conventional bulk-fill composites. Repair flexural strength varied by material and repair strategy, with notable interaction effects observed. These findings highlight important differences in mechanical and polymerization performance among bulk-fill composites under controlled laboratory conditions, warranting further clinical validation.
Acknowledgement: Not applicable.
Funding Statement: The authors received no specific funding for this study.
Author Contributions: Laila Saud Alrakhees conceptualized, contributed to the literature search, and drafted the initial manuscript. Sultan Binalrimal critically reviewed and drafted the final manuscript, assisted in statistical analysis and provided technical editing. All authors reviewed and approved the final version of the manuscript.
Availability of Data and Materials: Material Safety Data Sheets and technical data sheets are available from manufacturers upon request. Raw data and statistical outputs are available from the corresponding author upon reasonable request.
Ethics Approval: This in vitro study received Institutional Review Board (IRB) approval from Riyadh Elm University (FPGRP/2024/828/1155/1079). No human subjects or clinical data were involved.
Conflicts of Interest: The authors declare no conflicts of interest.
How to Cite this Article
References
- Khan AA, AlKhureif AA, Mohamed BA, Bautista LSJ. Enhanced mechanical properties are possible with urethane dimethacrylate-based experimental restorative dental composite. Mater Res Express. 2020;7(10):105307. doi:10.1088/2053-1591/abbf7f. DOI
- Chesterman J, Jowett A, Gallacher A, Nixon P. Bulk-fill resin-based composite restorative materials: a review. Br Dent J. 2017;222(5):337–44. doi:10.1038/sj.bdj.2017.214; 28281590 DOI
- Veloso SRM, Lemos CAA, de Moraes SLD, do Egito Vasconcelos BC, Pellizzer EP, de Melo Monteiro GQ. Clinical performance of bulk-fill and conventional resin composite restorations in posterior teeth: a systematic review and meta-analysis. Clin Oral Investig. 2019;23(1):221–33. doi:10.1007/s00784-018-2429-7; 29594349 DOI
- Sartawi SY, AbuSidu Z, El-Qawasmi Y, Salim NA. In vitro analysis of flowable and high viscosity bulk fill composite versus conventional composite in core build up of endodontically treated teeth. Sci Rep. 2024;14(1):28013. doi:10.1038/s41598-024-73108-1. DOI
- Kishan K, Solanki N, Saklecha P, Parikh M. Comparison of fiber-reinforced composite and nanohybrid resin impregnated with glass fibers as postendodontic restoration in molars—a clinical study. J Conserv Dent. 2021;24(5):514. doi:10.4103/jcd.jcd_147_21. DOI
- Gonçalves F, de Paiva Campos LM, Rodrigues-Júnior EC, Costa FV, Marques PA, Francci CE, et al. A comparative study of bulk-fill composites: degree of conversion, post-gel shrinkage and cytotoxicity. Braz Oral Res. 2018;32:e17. doi:10.1590/1807-3107bor-2018.vol32.0017; 29538479 DOI
- Rezaei S, Abbasi M, Sadeghi Mahounak F, Moradi Z. Curing depth and degree of conversion of five bulk-fill composite resins compared to a conventional composite. Open Dent J. 2019;13(1):422–9. doi:10.2174/1874210601913010422. DOI
- Monteiro V, Taguchi C, Machado G, Silva B, Bernardon K, Junior M. Bulk-fill composite restorations step-by-step description of clinical restorative techniques case reports. Odovtos Int J Dent Sc. 2019;21(2):23–31. doi:10.15517/ijds.v21i2.36681. DOI
- de Menezes AJO, do Nascimento Barbosa L, Leite JVC, Barbosa LMM, Montenegro RV, Dantas RVF, et al. Clinical outcomes of bulk-fill resin composite restorations: a 10-year mapping review and evidence gap map. J Esthet Restor Dent. 2025;37(4):920–33. doi:10.1111/jerd.13339; 39462873 DOI
- Garoushi S, Säilynoja E, Vallittu PK, Lassila L. Physical properties and depth of cure of a new short fiber reinforced composite. Dent Mater. 2013;29(8):835–41. doi:10.1016/j.dental.2013.04.016; 23726127 DOI
- Jafarnia S, Valanezhad A, Shahabi S, Abe S, Watanabe I. Physical and mechanical characteristics of short fiber-reinforced resin composite in comparison with bulk-fill composites. J Oral Sci. 2021;63(2):148–51. doi:10.2334/josnusd.20-0436; 33504755 DOI
- Attik N, Colon P, Gauthier R, Chevalier C, Grosgogeat B, Abouelleil H. Comparison of physical and biological properties of a flowable fiber reinforced and bulk filling composites. Dent Mater. 2022;38(2):e19–30. doi:10.1016/j.dental.2021.12.029; 34961643 DOI
- Elsharawy RM, Elawsya ME, Abdallah AM, Elembaby AE. Polymerization efficiency of different bulk-fill resin composites cured by monowave and polywave light-curing units: a comparative study. Quintessence Int. 2024;55(4):264. doi:10.3290/j.qi.b4984231; 38362702 DOI
- Rajak D, Pagar D, Menezes P, Linul E. Fiber-reinforced polymer composites: manufacturing, properties, and applications. Polymers. 2019;11(10):1667. doi:10.3390/polym11101667; 31614875 DOI
- Moldovan M, Balazsi R, Soanca A, Roman A, Sarosi C, Prodan D, et al. Evaluation of the degree of conversion, residual monomers and mechanical properties of some light-cured dental resin composites. Materials. 2019;12(13):2109. doi:10.3390/ma12132109; 31262014 DOI
- Hayashi J, Tagami J, Chan D, Sadr A. New bulk-fill composite system with high irradiance light polymerization: integrity and degree of conversion. Dent Mater. 2020;36(12):1615–23. doi:10.1016/j.dental.2020.10.012; 33168226 DOI
- Alrahlah A, Khan R, Al-Odayni AB, Saeed WS, Bautista LS, Vohra F. Evaluation of synergic potential of rGO/SiO2 as hybrid filler for BisGMA/TEGDMA dental composites. Polymers. 2020;12(12):3025. doi:10.3390/polym12123025. DOI
- de Jager N, Münker TJAG, Guilardi LF, Jansen VJ, Sportel YGE, Kleverlaan CJ. The relation between impact strength and flexural strength of dental materials. J Mech Behav Biomed Mater. 2021;122:104658. doi:10.1016/j.jmbbm.2021.104658; 34214922 DOI
- Khan AA, Zafar MS, Fareed MA, AlMufareh NA, Alshehri F, AlSunbul H, et al. Fiber-reinforced composites in dentistry—an insight into adhesion aspects of the material and the restored tooth construct. Dent Mater. 2023;39(2):141–51. doi:10.1016/j.dental.2022.12.003. DOI
- Oksanen V, Bijelic-Donova J, Vallittu PK, Lassila L, Garoushi S. Two different short fiber-reinforced resin composites for extensive MOD cavities in premolars and molars. Clin Oral Investig. 2025;29(10):462. doi:10.1007/s00784-025-06562-4; 40960634 DOI
- Abdulhameed NF. Quantitative fractographic analysis to measure the fracture toughness of dental resin composites [dissertation]. Gainesville, FL, USA: University of Florida; 2019.
- Khan AA, Al-Kheraif AA, Mohamed BA, Perea-Lowery L, Säilynoja E, Vallittu PK. Influence of primers on the properties of the adhesive interface between resin composite luting cement and fiber-reinforced composite. J Mech Behav Biomed Mater. 2018;88:281–7. doi:10.1016/j.jmbbm.2018.08.050; 30196183 DOI
- Khan AA, Mohamed BA, Al-Shamrani SS, Ramakrishnaiah R, Perea-Lowery L, Säilynoja E, et al. Influence of monomer systems on the bond strength between resin composites and polymerized fiber-reinforced composite upon aging. J Adhes Dent. 2019;21:509–16. doi:10.1016/j.jmbbm.2018.08.050. DOI
- Deliperi S, Bardwell DN. Reconstruction of nonvital teeth using direct fiberreinforced composite resin: a pilot clinical study. J Adhes Dent. 2009;11(1):71–8.
- Jordehi AY, Abdollahi S, Golshahirad G, Nouri A. Effect of adhesive type and silane application on the repair bond strength of aged bulk-fill composites. J Dent Mater Tech. 2025;14(3):128–34.
- Tohidkhah S, Jin J, Zhang A, Aregawi W, Morvaridi-Farimani R, Daisey EE, et al. Post-failure analysis of model resin-composite restorations subjected to different chemomechanical challenges. Dent Mater. 2024;40(6):889–96. doi:10.1016/j.dental.2024.04.005; 38692997 DOI
- Kaur G, Bansal RK, Bansal M, Bansal D, Garg R, Singla S, et al. Evaluation of marginal adaptation of SDR plus, fiber-reinforced and nanofilled composites in endodontically treated teeth: a scanning electron microscopic study. Cureus. 2024;16(10):e70745. doi:10.7759/cureus.70745; 39493132 DOI
- Chadgal S, Farooq R, Purra AR, Ahanger FA. Evaluation and comparison of fracture resistance of two low-viscosity bulk-fill resin-based restorative materials. J Adv Med Dent Sci Res. 2020;8(5):137–40.
- Garoushi S, Säilynoja E, Frater M, Keulemans F, Vallittu PK, Lassila L. A comparative evaluation of commercially available short fiber-reinforced composites. BMC Oral Health. 2024;24(1):1573. doi:10.1186/s12903-024-05267-6; 39736654 DOI