Abstract
Keywords: Combined periodontal-endodontic lesions; minocycline hydrochloride ointment; root canal injection; Vitapex paste
Combined periodontal-endodontic lesions are a common chronic infectious disease of the oral cavity, mainly defined as the periodontal destruction of the affected teeth accompanied by pulpitis. Periodontal and dental pulp tissues communicate and interact with each other through collateral branch root canal, dentinal tubules and apical foramen, so lesions or infections on one party may spread to the other, leading to combined lesions [1,2]. Patients with combined periodontal-endodontic lesions often suffer from varying degrees of periodontal pocket formation, pocket wall inflammation, gingival bleeding and alveolar bone resorption. If no effective treatment measures are taken promptly, the inflammatory reaction mediated by bacteria and plaque may extend to the subgingival region, involving the deep gingival tissue and causing tooth loosening or displacement, which has a negative impact on the daily life and physical and mental health of patients [3,4].
Removing dental plaque and calculus on the root surface, and eliminating or inhibiting anaerobic bacteria are the key in the treatment of combined periodontal-endodontic lesions. Combined periodontal-endodontic lesions were often treated with antibiotics previously, but antibiotics alone could not achieve satisfactory results due to the special periodontal environment. Iodoform-zinc oxide eugenol (ZOE) paste and Vitapex paste are both commonly-used root canal filling materials, and they have been widely applied in the repair of apical foramen destruction, apexification and root canal therapy of deciduous teeth, obtaining good results [5,6].
Recent studies have provided new insights into the role of microRNAs in regulating periodontal inflammation and tissue remodeling. The study showed that miRNAs such as miR 7, miR 21 and miR 100 modulate cytokine activity and the RANKL and OPG signaling pathways, thereby influencing osteoclast and osteoblast functions within periodontal tissues. It also demonstrated that the dynamic expression of these miRNAs in gingival crevicular fluid reflects local inflammatory burden and tissue remodeling activity, suggesting their involvement in both the progression and the repair of periodontal lesions [7]. In addition, recent periodontal research has linked dysregulated miRNAs with vascular inflammatory responses, oxidative stress and impaired endothelial function, which are biological processes closely associated with the destructive mechanisms of periodontitis and related endodontic involvement [8]. These findings provide a more refined molecular framework for understanding the inflammatory and tissue-level interactions underlying combined periodontal endodontic lesions.
Clinically, both Vitapex paste and iodoform ZOE paste are widely used intracanal filling materials, yet their differences in antibacterial activity, sealing capacity and tissue responses may lead to distinct therapeutic outcomes in combined periodontal endodontic lesions. However, despite the clinical relevance of these lesions and the growing understanding of their biological mechanisms, comparative evidence evaluating the therapeutic performance of these two materials remains limited. Therefore, we compared the clinical effects of iodoform ZOE paste and Vitapex paste in patients with combined periodontal endodontic lesions, with the aim of providing updated biological support and reliable clinical evidence to guide material selection in clinical practice.
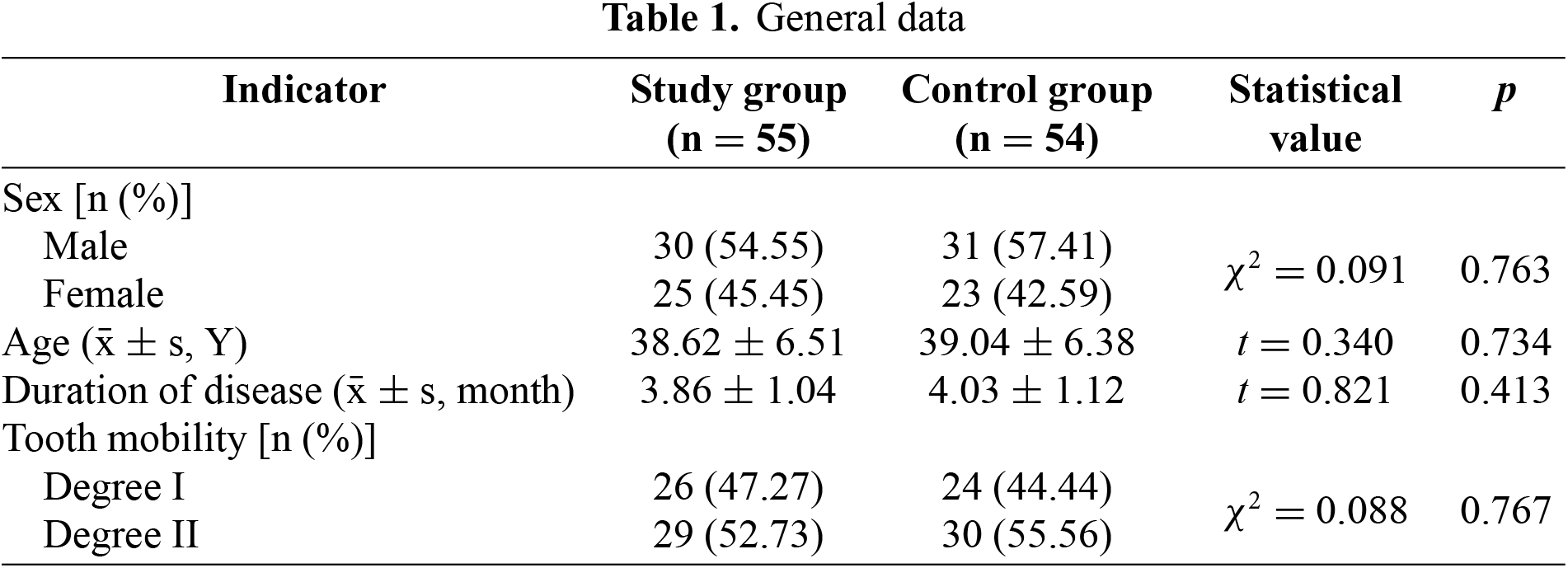
A total of 109 patients with combined periodontal-endodontic lesions treated in our hospital from October 2020 to October 2022 were selected and divided into control group (n = 54) and study group (n = 55) using a random number table. The data were well-balanced and comparable between the two groups (p > 0.05) (Table 1).
2.2. Sample size justification
This study adopted a pragmatic, prospective randomized controlled design. The anticipated number of participants was initially estimated based on the expected patient volume during the recruitment period and effect sizes reported in previous studies on similar periodontal–endodontic conditions. However, the available preliminary evidence was not sufficiently precise to allow a formal a priori sample size calculation. Therefore, all eligible patients treated within the predefined period were consecutively enrolled and randomized. To evaluate the adequacy of the achieved sample size, post-hoc power analyses were conducted for two major outcomes, probing depth (PD) and IL-1β. These outcomes reflect the core clinical and biological therapeutic targets of periodontal and endodontic involvement. Based on the observed effect sizes, the statistical power exceeded 0.80 for both probing depth and IL-1β at a significance level of 0.05. These results indicate that the sample size was sufficient to detect clinically meaningful differences in the main outcomes of interest.
2.3. Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) Patients diagnosed with combined periodontal–endodontic lesions based on clinical examination, periodontal probing, pulp vitality testing and radiographic findings [9], (2) patients presenting with symptoms such as gingival bleeding, redness and swelling, occlusal pain, and with a PD of 3–10 mm, (3) presence of symptoms or radiographic signs of pulpal or periapical involvement, (4) first-time treatment, aged between 18 and 65 years, and in good systemic health without acute infection or uncontrolled systemic disease, (5) no history of periodontal treatment, root canal therapy or systemic antibiotic use within the previous 3 months, (6) ability and willingness to comply with study procedures and follow-up.
The exclusion criteria were: (1) Patients with root canal rupture or radiographically confirmed periapical cysts, (2) patients with known allergy to any of the investigational materials, (3) patients with a history of dental aesthetic restorative procedures that may affect periodontal assessment, (4) patients with alveolar bone resorption greater than one-half of the root length as shown on X-ray examination, (5) patients who had used antibiotics or corticosteroid medications within the past month, (6) patients with rheumatic immune system diseases, endocrine disorders or other systemic diseases that may influence periodontal status, (7) patients with other acute or chronic infectious diseases.
Periodontal therapy and root canal therapy were performed in both groups. (1) Periodontal therapy: X-ray examination was first performed to observe the periapical condition, and range and degree of periodontal destruction. Subgingival and supragingival scaling was provided according to individual conditions. Then the periodontal pocket was washed alternately and repeatedly with normal saline and 3% hydrogen peroxide solution, and the exudate in the periodontal pocket was absorbed with cotton balls. Finally, an appropriate amount of minocycline hydrochloride ointment (Sunstar INC, Japan, Registration Certificate No. H20150106, specification: 0.5 g) was slowly injected into the periodontal pocket until it slightly overflowed. It was forbidden to gargle or eat within 1 h after treatment. The treatment lasted for eight weeks, once a week.
(2) Root canal therapy: Root canal therapy was performed simultaneously with periodontal therapy. After pulp opening, pulp extraction and root canal preparation using K files, the root canal was ultrasonically washed and sealed with drugs for 7–10 d until symptoms disappeared. Then the root canal was dried and filled with iodoform-ZOE paste (prepared by iodoform and zinc oxide powder at 5:1 with eugenol) in control group and with Vitapex paste (Morita, Japan) in study group till 1/3 of the apex after there was no exudation or peculiar smell. After the whole root canal was confirmed to be fully filled with the paste, it was sealed with gutta-percha points. Following eight weeks of treatment, the paste was removed and the root canal was filled permanently. Moreover, the two groups of patients were required to gargle after three meals, keep the oral cavity clean, and receive tooth-clicking exercise and regular review.
2.5. Observation of indicators
(1) Clinical efficacy: After eight weeks of treatment, the clinical efficacy was evaluated in the two groups. The evaluation criteria were as follows: Markedly effective: complete disappearance of symptoms such as gingival bleeding, redness and swelling, and occlusal pain, decline in PD ≥2 mm, and no loosening and spontaneous pain of the affected teeth. Effective: Significant improvement of symptoms such as gingival bleeding, redness and swelling, and occlusal pain, 1 mm < decline in PD <2 mm, and slight loosening but no spontaneous pain of the affected teeth. Ineffective: No significant improvement of clinical symptoms, PD, loosening/spontaneous pain of the affected teeth and other signs. Total effective rate = markedly effective rate + effective rate.
(2) Adverse reactions: The incidence of local itching, oral foreign body sensation, and gingival bleeding was recorded in the two groups.
(3) Periodontal status: Gingival index (GI), plaque index (PLI), clinical attachment level (CAL) and PD were compared between the two groups before treatment and at eight weeks after treatment. GI [10]: 0 points (normal gingival texture and color), 1 point (slightly ruddy color and mild inflammation of the gingiva), 2 points (significantly ruddy color and moderate inflammation of the gingiva), and 3 points (gingival ulcer or redness, and severe inflammation). PLI [11]: 0 points (no plaque at the gingival margin), 1 point (no plaque at the gingival margin found by visual inspection, but a small amount of plaque scraped out with the probe tip), 2 points (a moderate amount of plaque at the gingival margin found by both visual inspection and probing), and 3 points (a large amount of tartar at the gingival margin, on the adjacent surface and in the gingival sulcus found by both visual inspection and probing). CAL was defined as the distance from the cementoenamel junction to the periodontal pocket bottom, and PD referred to the distance from the gingival margin to the periodontal pocket bottom or from the upper gingival margin to the gingival sulcus bottom.
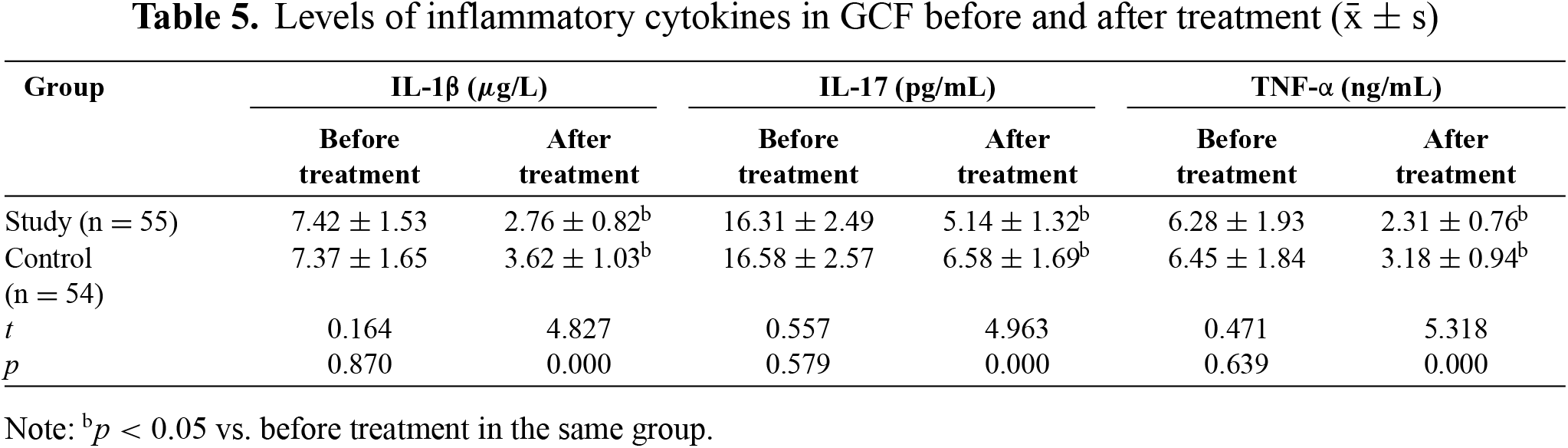
(4) Levels of inflammatory cytokines in gingival crevicular fluid (GCF): GCF was harvested before treatment and at eight weeks after treatment and centrifuged at 3500 r/min for 15 min. Then the supernatant was collected to measure the levels of tumor necrosis factor-α (TNF-α), interleukin-1β (IL-1β) and IL-17 by enzyme-linked immunosorbent assay.
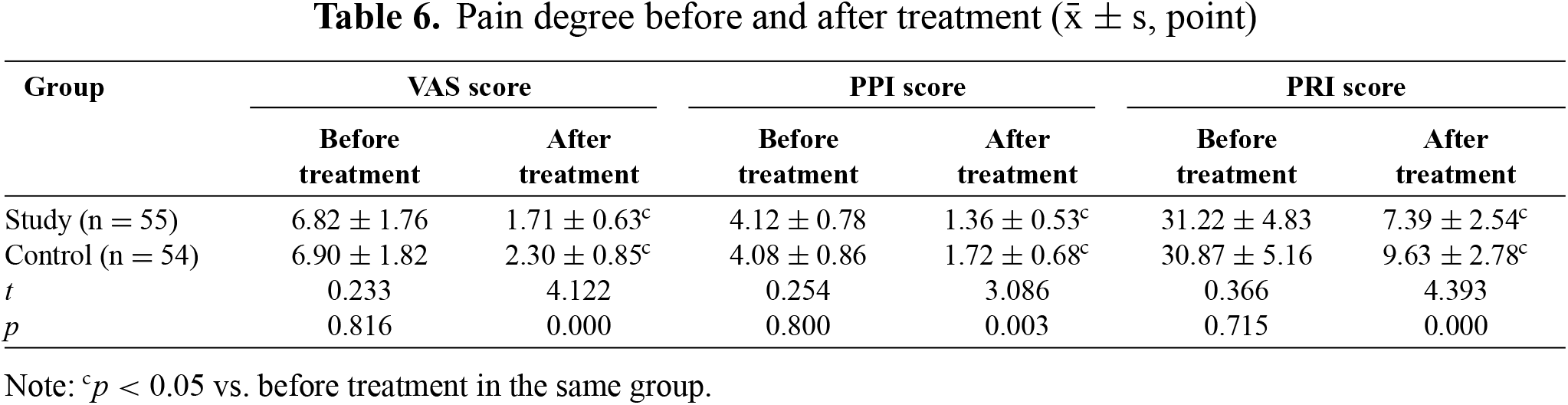
(5) Degree of pain: Before treatment and at eight weeks after treatment, the degree of pain was assessed using the short-form McGill pain questionnaire (SF-MPQ) [12], which consisted of visual analogue scale (VAS) [13], pain rating index (PRI) and present pain intensity (PPI). The higher the VAS score (0–10 points), the severer the pain. PPI had six grades: 0 points (no pain), 1 point (mild pain), 2 points (uncomfortable pain), 3 points (great pain), 4 points (terrible pain) and 5 points (severe pain). PRI covered 15 items in total, including four kinds of emotions (boredom, fear, weakness and suffering) and 11 kinds of pain properties such as tenderness, burning pain, tingling pain and knife-like pain. Each item was scored 0–3 points from “none” to “severe”, the total score was 0–45 points, and a higher score corresponded to a higher degree of pain.
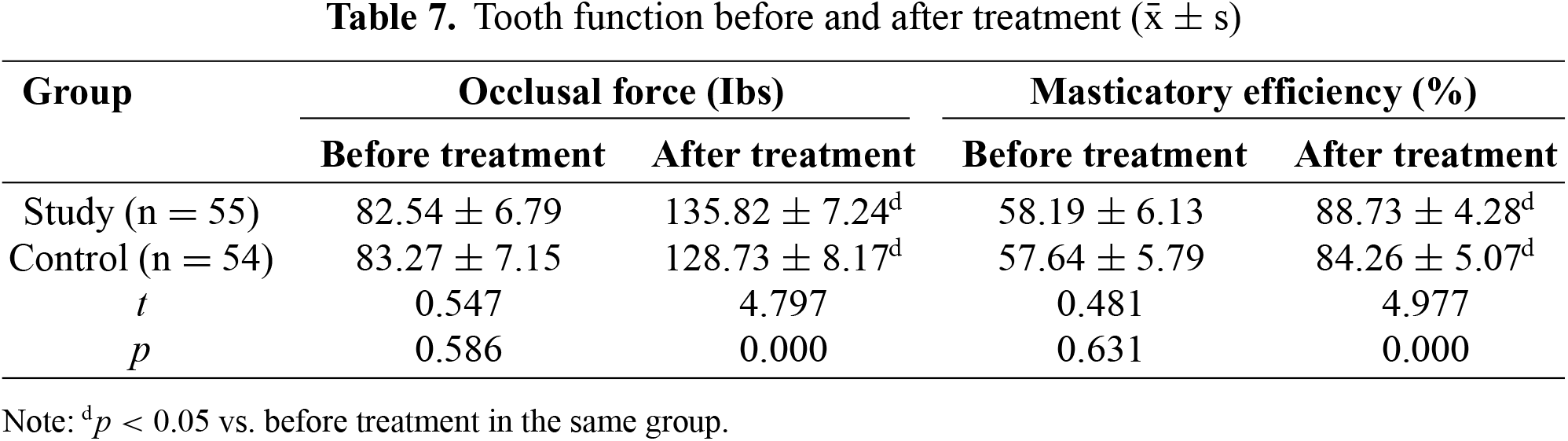
(6) Tooth function: The occlusal force and masticatory efficiency were compared between the two groups before treatment and at 8 weeks after treatment. The occlusal force was measured with an occlusometer (YHL001). To detect the masticatory efficiency, the patient was instructed to chew 5 g of peeled and fried peanuts, 20 times by each side of the teeth, and then the chews were filtered with a 200-mesh sieve and weighed. Masticatory efficiency = weight of filtered chews/weight of peanuts before chewing.
SPSS 23.0 software was used for statistical analysis. Normality of continuous variables was assessed using the Shapiro Wilk test. All variables showed normal distribution, so between group comparisons were conducted using independent samples t tests. The count data (clinical efficacy and adverse reactions) were described by [n (%)] and subjected to the χ2 test. The rank sum test was used for the ranked data. p < 0.05 was considered a statistically significant difference.
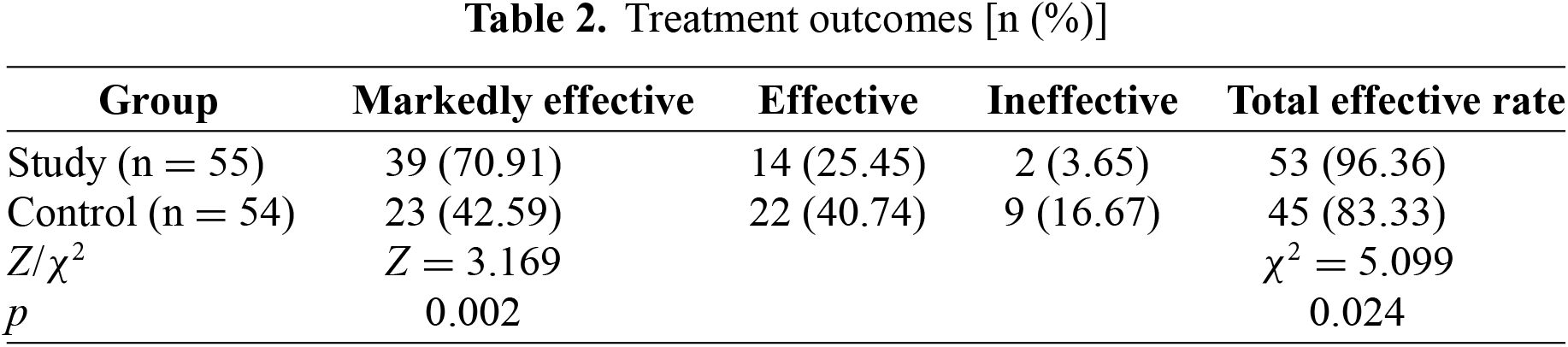
The total effective rate of the study group was higher than that of the control group (p < 0.05) (Table 2).
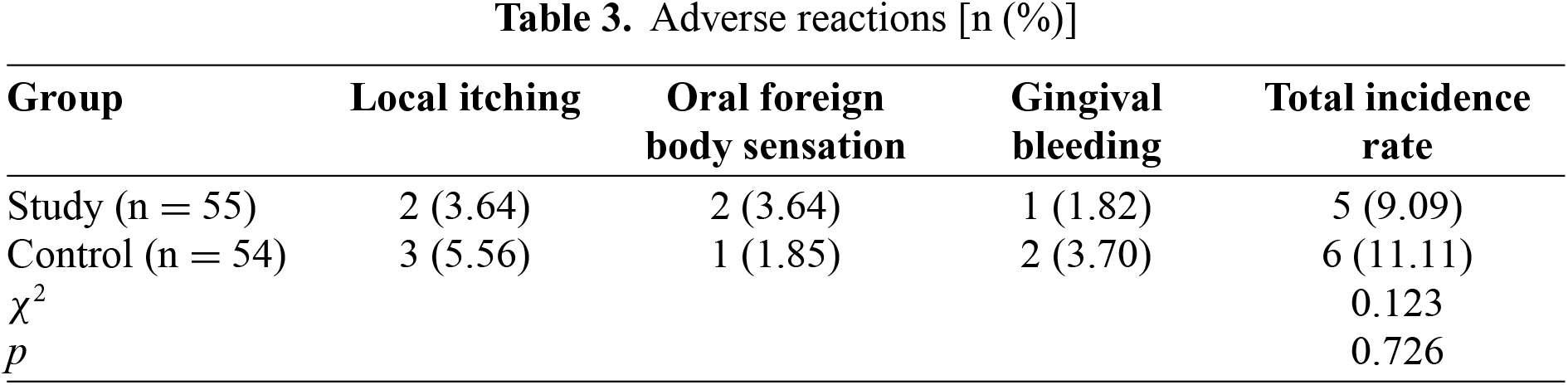
There was no significant difference in the incidence rates of adverse reactions between the two groups (p > 0.05) (Table 3).
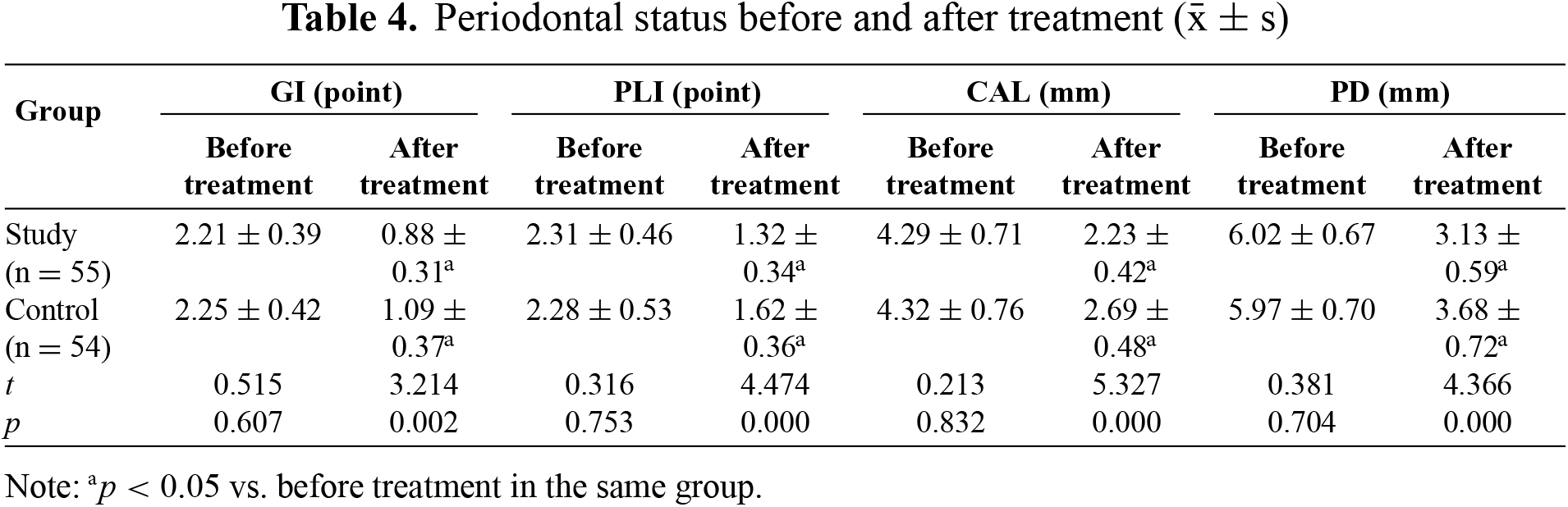
3.3. Periodontal status before and after treatment
After treatment, GI, PLI, CAL and PD all declined in both groups compared with those before treatment, and the changes were more significant in the study group than those in the control group (p < 0.05) (Table 4).
3.4. Levels of inflammatory cytokines in GCF before and after treatment
After treatment, the levels of IL-1β, IL-17 and TNF-α all declined in both groups compared to those before treatment, and they were lower in the study group than those in the control group (p < 0.05) (Table 5).
3.5. Pain degree before and after treatment
After treatment, the scores of VAS, PPI and PRI all declined in both groups compared to those before treatment, and they were lower in the study group than those in the control group (p < 0.05) (Table 6).
3.6. Tooth function before and after treatment
Both occlusal force and masticatory efficiency were enhanced in the two groups after treatment, and they were higher in the study group than those in the control group (p < 0.05) (Table 7).
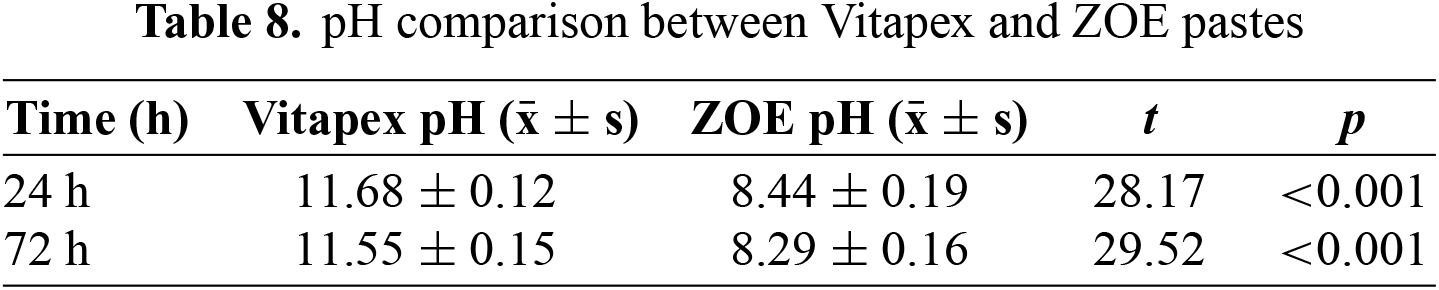
3.7. Comparative physicochemical evaluation of root canal materials
To compare the physicochemical characteristics of Vitapex paste and ZOE paste, pH value, antibacterial performance and minocycline release profile were analyzed. As shown in Table 8, the pH of Vitapex remained above 11.5 throughout the 72 h incubation, significantly higher than that of ZOE paste (p < 0.05), indicating a stronger alkalinity conducive to antibacterial activity and dentin bridge formation.
Agar diffusion assay showed that Vitapex produced a larger inhibition zone against E. faecalis (19.7 ± 1.2 mm) than ZOE paste (14.2 ± 0.9 mm), supporting its superior antibacterial effect. Similarly, minocycline ointment exhibited sustained release, reaching 72% cumulative release at 24 h (Figure 1), indicating favorable local drug delivery properties.
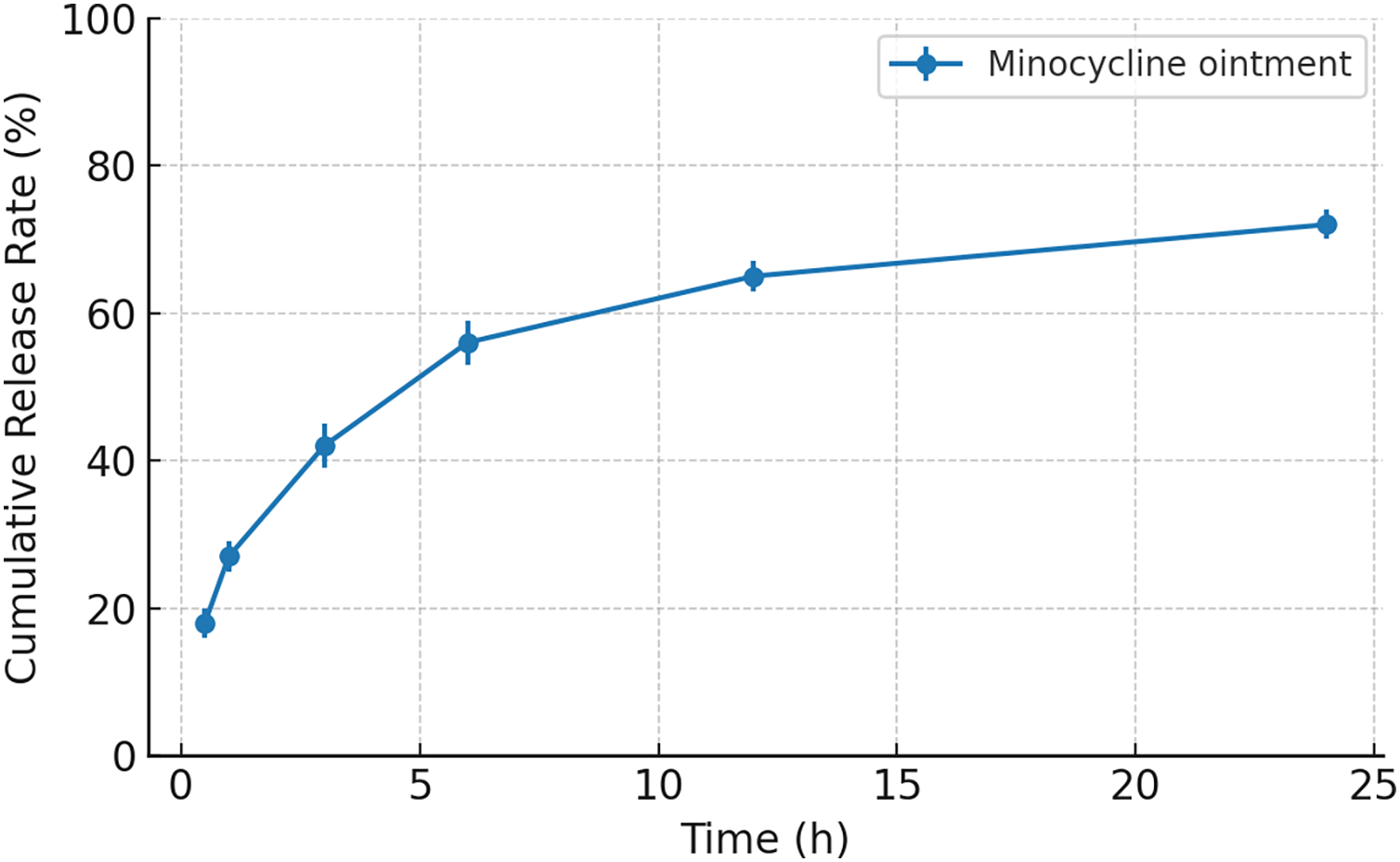
Figure 1. Cumulative minocycline release profile in PBS over 24 h (n = 3). Error bars represent standard deviation
This study demonstrated that Vitapex paste combined with minocycline hydrochloride ointment provided superior clinical outcomes compared with iodoform-ZOE paste, with greater improvements in periodontal indices, inflammatory cytokines, pain scores and tooth function.
SEM imaging of Vitapex has shown homogeneous dispersion and good biocompatibility due to its polysiloxane-based matrix [14]. FTIR analysis of calcium hydroxide-based sealers has also demonstrated strong hydroxyl group peaks related to their antimicrobial and mineralizing potential [15]. Furthermore, a sustained-release profile of minocycline in a simulated physiological environment was demonstrated in the study by Patel et al. [16] through dissolution testing in PBS, confirming the formulation’s controlled-release capability. Complementary structural characterization via FTIR of a minocycline-loaded hydrogel system further supports the premise of material-mediated stability and functional release behavior [17].
Combined periodontal-endodontic lesions have complex pathogenesis, which may be related to dental plaque infection, Bacteroides gingivalis infection, immunity, psychology, environment, heredity and other factors [18]. Periodontal lesions and dental pulp lesions interact with each other, and pulp necrosis or lesions can affect periodontal tissues through the apical foramen. Moreover, the plaque on the root surface can also lead to pathological changes in the dental pulp. When periodontitis invades the apical foramen, dental pulp lesions may also be induced [19,20]. Only by simultaneously treating periodontal lesions and dental pulp lesions can ideal clinical effects be achieved on patients with combined periodontal-endodontic lesions.
Inflammation of granulation tissues induced by continuous stimulation of pathogenic microorganisms is the major pathological feature of combined periodontal-endodontic lesions, which can destroy periodontal tissues, and cause sensitive pain and even tooth loss, affecting tooth function [21]. With ability to quickly and effectively eliminate necrotic pulp tissues, root canal therapy is commonly used for patients with combined periodontal-endodontic lesions. However, completely removing pathogenic microorganisms in the root canal by root canal therapy alone remains difficult, so it is necessary to actively search for disinfection drugs to contribute to the complete removal of pathogenic microorganisms. Characterized by a broad antibacterial spectrum, high fat solubility and strong permeability, minocycline hydrochloride ointment is a common local sustained-release drug in clinic, and it has a good antibacterial effect and can kill and inhibit pathogenic microorganisms in the oral cavity such as Eikenella corrodens, Actinobacillus actinomycetemcomitans, Fusobacterium and Spirochete. After being injected into the periodontal pocket, minocycline hydrochloride ointment can slowly release minocycline and maintain a high drug concentration in local lesions for a long time, exerting a good sterilization effect [16,22]. Meanwhile, minocycline hydrochloride ointment can chelate with zinc ions and calcium ions to inhibit collagenase activation, promote slight demineralization of the root surface of the affected tooth, and expose the cementum collagen fiber at the lesion site, thereby facilitating the growth and extension of periodontal ligament cells [23]. A long-term sterile state of the root canal is required for a perfect root canal therapy, so continuous disinfection and bacteriostasis are the necessary characteristics of root canal fillers. Iodoform-ZOE paste is a commonly used root canal filling material in clinical practice, and it has obvious inhibitory effects on Lactobacillus, Staphylococcus epidermidis and other bacteria, which can achieve continuous disinfection and bacteriostasis in the root canal [24,25]. However, eugenol in iodoform-ZOE paste has certain cytotoxicity, which will adversely affect the normal absorption of root tissue, resulting in abnormal development of permanent tooth enamel and affecting the therapeutic effect. Besides, the root canal needs to be expanded when iodoform-ZOE paste is used, and it is difficult to control the tightness of filling with poor tissue absorption, which is not conducive to the prognosis of patients.
Vitapex paste is mainly composed of calcium hydroxide, iodoform and polysiloxane oil. After reaction with some pathogenic microorganisms and tissue fluid, iodoform will slowly release free iodine and bind to amino groups in protein, achieving continuous sterilization [26]. Calcium hydroxide has antiseptic, sterilization and bacteriostatic effects and can also stimulate the formation of calcified tissue [27]. As an excipient carrier, polysiloxane oil can enhance the histocompatibility and absorbability of iodoform and calcium hydroxide, improving both bacteriostatic and anti-inflammatory effects. In this study, iodoform-ZOE paste and Vitapex paste were compared in patients with combined periodontal-endodontic lesions. It was found that the total effective rate of 8-week treatment in study group (96.36%) was higher than that in control group (83.33%). After treatment, study group had lower GI, PLI, CAL, PD and scores of VAS, PPI and PRI than control group, suggesting that Vitapex paste has better clinical efficacy on patients with combined periodontal-endodontic lesions, and it can effectively relieve the clinical symptoms and pain. The possible reason is that the filling of injectable Vitapex paste is a simple operation and can increase the root canal filling pressure, making the filling materials closely fit the root canal wall, and eliminating the inflammation and exudation of the root canal, so as to quickly relieve the clinical symptoms and pain of patients, improve the periodontal status, and enhance the clinical efficacy.
Combined periodontal-endodontic lesions are not only infectious lesions but also systemic inflammatory host responses. Chronic inflammatory responses can be generated after the affected tooth is mixed infected by multiple pathogenic microorganisms, and then chronic inflammation will stimulate the periodontal tissue and induce the release of inflammatory cytokines such as IL-1β, IL-17 and TNF-α [28,29]. Among them, IL-1β and IL-17 are common pro-inflammatory factors able to up-regulate the expressions of IL-6 and IL-8, causing inflammatory cascade reactions and worsening inflammatory injuries [30]. TNF-α with various biological activities can reduce the alkaline phosphatase activity of periodontal ligament fiber cells and inhibit the transformation of periodontal ligament fiber cells, thus destroying alveolar bone [31]. In this study, the levels of IL-1β, IL-17 and TNF-α in study group were lower than those in control group after treatment, and the tooth function was also better than that in control group, suggesting that injection of Vitapex paste combined with minocycline hydrochloride ointment can effectively alleviate the inflammatory response and improve the tooth function of patients with combined periodontal-endodontic lesions.
Recent evidence suggests that oxidative stress plays a key role in the progression of periodontal inflammation. Excessive production of reactive oxygen species can damage periodontal ligament cells, promote lipid peroxidation, impair mitochondrial function and amplify inflammatory cytokine release [32]. IL 1β and TNF α further enhance ROS generation, forming a cycle that accelerates periodontal tissue breakdown [33]. The greater reductions in inflammatory cytokines observed in the study group may therefore be associated with improved modulation of oxidative stress, which contributes to better periodontal tissue stability and functional recovery.
Minocycline hydrochloride ointment is a slow-release antibacterial drug, which can form a layer of thin film when contacted with water in the local periodontal region, and slowly release the drug to maintain a local high drug concentration for a long time, thereby achieving sustained and strong antibacterial effects, suppressing inflammatory responses and enhancing periodontal tissue healing [17,34]. Polysiloxane oil in Vitapex paste possesses good permeability and fluidity, which can ensure complete filling of collateral branch root canal and make calcium hydroxide, iodoform and other drugs penetrate the affected tooth tissue, thereby exerting a sustained bactericidal effect. Moreover, polysiloxane oil can stimulate the formation of calcified tissues and opening of dentin tubules, so that minocycline hydrochloride ointment can better kill bacteria in the dental pulp, repairing periodontal tissues and improving tooth function [35]. In this study, adverse reactions such as mild local itching, oral foreign body sensation and gingival bleeding occurred in a small number of patients, but they had no impact on the treatment, and there was no significant difference in the incidence of adverse reactions between the two groups. It can be seen that injection of Vitapex paste combined with minocycline hydrochloride ointment is safe in the treatment.
This study has several limitations that should be acknowledged. First, it was a single center randomized controlled trial with a relatively modest sample size, which may limit the generalizability of the findings to broader populations and different clinical settings. Second, the follow up period was restricted to short term clinical and inflammatory outcomes, and long-term periodontal stability and endodontic healing were not evaluated. Third, although key clinical and biomarker parameters were assessed, additional mechanistic indicators such as microbiological profiles or cytokine dynamics were not included and may provide deeper insights into treatment response. Finally, blinding of operators and patients was not feasible due to the nature of the interventions, which may introduce potential performance bias despite standardized procedures. Future studies with multimodal evaluation and extended follow up are warranted to further validate these findings.
In conclusion, root canal injection of Vitapex paste combined with minocycline hydrochloride ointment can effectively reduce inflammatory cytokines in GCF, improve periodontal parameters, enhance tooth function and alleviate pain with good safety. By providing sustained antibacterial action and supporting periodontal tissue healing, this combined approach demonstrates stronger therapeutic benefits for managing combined periodontal–endodontic lesions.
Acknowledgement: This study was financially supported by Grand No. 81400521.
Funding Statement: This study was financially supported by Grand No. 81400521.
Author Contributions: Study conception and design, and significant manuscript revision: Shiliang Guo; Data collection, analysis and interpretation of results, and manuscript drafting: Jingjing Nie and Jiafei Feng. All authors reviewed the results and approved the final version of the manuscript.
Availability of Data and Materials: Data available on request from the authors.
The data that support the findings of this study are available from the corresponding author, Shiliang Guo, upon reasonable request.
Ethics Approval: Not Applicable.
Conflicts of Interest: The authors declare no conflicts of interest.
How to Cite this Article
References
- Song M, Kang M, Kang DR, Jung HI, Kim E. Comparison of the effect of endodontic-periodontal combined lesion on the outcome of endodontic microsurgery with that of isolated endodontic lesion: survival analysis using propensity score analysis. Clin Oral Investig. 2018;22(4):1717–24. doi:10.1007/s00784-017-2265-1; 29098442 DOI
- Jara CM, Pereira KKY, Maito FLDM, Adorno CG, Gomes MS. Impact of endodontic and periodontal diseases and treatments on the aorta and liver of obese and non-obese rats. Int Endod J. 2021;54(11):2074–85. doi:10.1111/iej.13601; 34351629 DOI
- Emara RS, Abou El Nasr HM, El Boghdadi RM. Evaluation of postoperative pain intensity following occlusal reduction in teeth associated with symptomatic irreversible pulpitis and symptomatic apical periodontitis: a randomized clinical study. Int Endod J. 2019;52(3):288–96. doi:10.1111/iej.13012; 30171777 DOI
- Nelson-Filho P, Ruviére DB, de Queiroz AM, de Paula-Silva FW, Silva RA, Lucisano MP, et al. Comparative Molecular analysis of gram-negative bacteria in primary teeth with irreversible pulpitis or periapical pathology. Pediatr Dent. 2018;40(4):259–64; 30345964
- Nishikawa Y, Matsuda S, Nakayasu Y, Toriya J, Yokoi Y, Shoumura M, et al. Reactions of the dentin-pulp complex to calcium hydroxide paste in rats. J Hard Tissue Biol. 2017;26(2):169–76. doi:10.2485/jhtb.26.169. DOI
- Pramila R, Muthu MS, Deepa G, Farzan JM, Rodrigues SJL. Pulpectomies in primary mandibular molars: a comparison of outcomes using three root filling materials. Int Endod J. 2016;49(5):413–21. doi:10.1111/iej.12478; 26059708 DOI
- Polizzi A, Alibrandi A, Lo Giudice A, Distefano A, Orlando L, Analazi AM, et al. Impact of periodontal microRNAs associated with alveolar bone remodeling during orthodontic tooth movement: a randomized clinical trial. J Transl Med. 2024;22(1):1155. doi:10.1186/s12967-024-05933-x; 39736760 DOI
- Polizzi A, Nibali L, Tartaglia GM, Isola G. Impact of nonsurgical periodontal treatment on arterial stiffness outcomes related to endothelial dysfunction: a systematic review and meta-analysis. J Periodontol. 2025;96(4):330–45. doi:10.1002/JPER.24-0422; 39549247 DOI
- Guo J, Li Y, Lin X, Yang X, Shi W, Lu X. Prognostic factors of combined periodontal and endodontic lesions: a retrospective study. Contrast Medium Mol Imag. 2022;2022(1):5042097. doi:10.1155/2022/5042097; 36051933 DOI
- El-Chami H, Younis A, Brignardello-Petersen R. Efficacy of oscillating rotating versus side-to-side powered toothbrushes on plaque and gingival index reduction: a systematic review. J Am Dent Assoc. 2021;152(2):115–26.e4. doi:10.1016/j.adaj.2020.10.002; 33358240 DOI
- Pinto TMP, de Freitas GC, Dutra DA, Kantorski KZ, Moreira CH. Frequency of mechanical removal of plaque as it relates to gingival inflammation: a randomized clinical trial. J Clin Periodontol. 2013;40(10):948–54. doi:10.1111/jcpe.12135; 23909568 DOI
- Melzack R. The short-form McGill pain questionnaire. Pain. 1987;30(2):191–7. doi:10.1016/0304-3959(87)91074-8; 3670870 DOI
- Phan N, Blome C, Fritz F, Gerss J, Reich A, Ebata T, et al. Assessment of pruritus intensity: prospective study on validity and reliability of the visual analogue scale, numerical rating scale and verbal rating scale in 471 patients with chronic pruritus. Acta Derm Venerol. 2012;92(5):502–7. doi:10.2340/00015555-1246; 22170091 DOI
- Okamoto M, Naito K, Duncan HF, Kinomoto Y, Kuriki N, Miura J, et al. Microstructural evaluation of the mineralized apical barrier induced by a calcium hydroxide paste containing iodoform: a case report. J Endod. 2024;50(2):243–51. doi:10.1016/j.joen.2023.10.013; 37918795 DOI
- Suwartini T, Santoso J, Widyarman AS, Ratnasari D. Efficacy of bioceramic and calcium hydroxide-based root canal sealers against pathogenic endodontic biofilms: an in vitro study. Contemp Clin Dent. 2022;13(4):322–30. doi:10.4103/ccd.ccd_198_21; 36687000 DOI
- Patel SK, Greene AC, Desai SM, Rothstein S, Basha IT, MacPherson JS, et al. Biorelevant and screening dissolution methods for minocycline hydrochloride microspheres intended for periodontal administration. Int J Pharm. 2021;596(1–2):120261. doi:10.1016/j.ijpharm.2021.120261; 33486044 DOI
- Wang X, Ma J, Zhu X, Wang F, Zhou L. Minocycline-loaded in situ hydrogel for periodontitis treatment. Curr Drug Deliv. 2018;15(5):664–71. doi:10.2174/1567201814666171120120421; 29165071 DOI
- Segura-Egea JJ, Martín-González J, del Carmen Jiménez-Sánchez M, Crespo-Gallardo I, Saúco-Márquez JJ, Velasco-Ortega E. Worldwide pattern of antibiotic prescription in endodontic infections. Int Dent J. 2017;67(4):197–205. doi:10.1111/idj.12287; 28417452 DOI
- Siqueira JF, Lenzi R, Hernández S, Alberdi JC, Martin G, Pessotti VP, et al. Effects of endodontic infections on the maxillary sinus: a case series of treatment outcome. J Endod. 2021;47(7):1166–76. doi:10.1016/j.joen.2021.04.002; 33864883 DOI
- Jahreis M, Soliman S, Schubert A, Connert T, Schlagenhauf U, Krastl G, et al. Outcome of non-surgical root canal treatment related to periodontitis and chronic disease medication among adults in age group of 60 years or more. Gerodontology. 2019;36(3):267–75. doi:10.1111/ger.12407; 31025786 DOI
- Tampi MP, Pilcher L, Urquhart O, Kennedy E, O’Brien KK, Lockhart PB, et al. Antibiotics for the urgent management of symptomatic irreversible pulpitis, symptomatic apical periodontitis, and localized acute apical abscess systematic review and meta-analysis—a report of the American Dental Association. J Am Dent Assoc. 2019;150(12):e179–216. doi:10.1016/j.adaj.2019.09.011; 31761029 DOI
- Xu L, Wang Y, Nguyen VT, Chen J. Effects of topical antibiotic prophylaxis on wound healing after flapless implant surgery: a pilot study. J Periodontol. 2016;87(3):275–80. doi:10.1902/jop.2015.150464; 26537369 DOI
- Shao W, Xiao F, Xu Z, Ren R, Wang Y, Wu Y. Treatment of severe periodontic-endodontic combined lesions with minocycline hydrochloride ointment combined with mineral trioxide aggregate. Exp Ther Med. 2018;16(2):1389–96. doi:10.3892/etm.2018.6341; 30116388 DOI
- Santos NCN, Ramos MESP, Ramos AFB, Cerqueira AB, Cerqueira EMM. Evaluation of the genotoxicity and cytotoxicity of filling pastes used for pulp therapy on deciduous teeth using the micronucleus test on bone marrow from mice (Mus musculus). Mutagenesis. 2016;31(5):589–95. doi:10.1093/mutage/gew026; 27251419 DOI
- Joseph R, Sasikumar M, Mammen J, Joseraj MG, Radhakrishnan C. Nonsurgical periodontal-therapy improves glycosylated hemoglobin levels in pre-diabetic patients with chronic periodontitis. World J Diabetes. 2017;8(5):213. doi:10.4239/wjd.v8.i5.213; 28572882 DOI
- Kwon W, Kim IH, Kang CM, Kim B, Shin Y, Song JS. Comparative study of pulpal responses to ProRoot MTA, Vitapex, and Metapex in canine teeth. J Dent Sci. 2021;16(4):1274–80. doi:10.1016/j.jds.2020.12.011; 34484596 DOI
- Sijini OT, Sabbagh HJ, Baghlaf KK, Bagher AM, El-housseiny AA, Alamoudi NM, et al. Clinical and radiographic evaluation of triple antibiotic paste pulp therapy compared to Vitapex pulpectomy in non-vital primary molars. Clin Exp Dent Res. 2021;7(5):819–28. doi:10.1002/cre2.434; 34060250 DOI
- Pérez-Serrano RM, Soza-Bolaños AI, Castillo-Valdés SN, Hernández-Valdez G, Mora-Izaguirre O, González-Dávalos ML, et al. Endodontic set sealer eluates promote cytokine production in human mononuclear and periodontal ligament cells. Aust Endod J. 2021;47(3):415–22. doi:10.1111/aej.12493; 33650775 DOI
- Garrido M, Cárdenas AM, Astorga J, Quinlan F, Valdés M, Chaparro A, et al. Elevated systemic inflammatory burden and cardiovascular risk in young adults with endodontic apical lesions. J Endod. 2019;45(2):111–5. doi:10.1016/j.joen.2018.11.014; 30711165 DOI
- Huang S, Song Z, Huang Q, Jiang L, Chen L, Wang R, et al. AIM2 inflammasome is critical for dsDNA-induced IL-1β secretion in human dental pulp cells. Inflammation. 2018;41(2):409–17. doi:10.1007/s10753-017-0697-z; 29178062 DOI
- Ghattas Ayoub C, Aminoshariae A, Bakkar M, Ghosh S, Bonfield T, Demko C, et al. Comparison of IL-1β, TNF-α, hBD-2, and hBD-3 expression in the dental pulp of smokers versus nonsmokers. J Endod. 2017;43(12):2009–13. doi:10.1016/j.joen.2017.08.017; 29033092 DOI
- Hosseini S, Diegelmann J, Folwaczny M, Frasheri I, Wichelhaus A, Sabbagh H, et al. Investigation of impact of oxidative stress on human periodontal ligament cells exposed to static compression. Int J Mol Sci. 2024;25(24):13513. doi:10.3390/ijms252413513; 39769281 DOI
- Liu W, Guo D. Oxidative stress in periodontitis and the application of antioxidants in treatment: a narrative review. Front Physiol. 2025;16:1485367. doi:10.3389/fphys.2025.1485367; 40488141 DOI
- Maia GV, Sousa CW, de Lima JCR, Vecchio JL, de Barros Silva PG, de Souza Carvalho ACG. Cyanoacrylate glue in socket repair: a comparative study. Br J Oral Maxillofac Surg. 2022;60(2):145–51. doi:10.1016/j.bjoms.2021.01.017; 34953568 DOI
- Wang Z, Nong J, Shultz RB, Zhang Z, Kim T, Tom VJ, et al. Local delivery of minocycline from metal ion-assisted self-assembled complexes promotes neuroprotection and functional recovery after spinal cord injury. Biomaterials. 2017;112(2):62–71. doi:10.1016/j.biomaterials.2016.10.002; 27744221 DOI